6 Answers sorted by
*
375The crux of your argument, that micro-gram level AL exposure has negative impacts, is based on the premature infant aluminum toxicity paper. It's a p-hacked piece of junk. They found no significant effect (P=0.39!!!) and then started analyzing subgroups until they got a p<0.05. Without adjusting for multiplicity, of course. Its implications would also only generalize to premature children. In addition, this study focuses on premature infants, not vaccine-age children. And blood AL levels were never taken! It's a bad paper and should be ignored.
On the other hand, this publication cites a paper noting that radio-labeled aluminum has 99.5% of injected aluminum being removed from the blood after 24 hours... but also that 50% is removed after an hour, and that it has a biological half-life of 7 years (!!??). Apparently, it mostly settles to the bones. This matches the 40-50mg total AL load figure I've seen elsewhere.
This brings us to Priest's paper, which actually explores the blood-brain barrier in regard to aluminum and it estimates... 8 micrograms of transfer from the blood to the brain per year. The brain has much lower levels of AL than the rest of the body. This implies that sudden spikes in blood aluminum levels simply won't have a major impact. Remember, aluminum can only cause brain damage if it reaches toxic levels. High blood AL only increases the speed at which brain AL levels increase. What really matters is the actual levels of brain AL, which is determined by long-term blood AL levels.
So let's look at chronic exposure. The average human consumes ~10mg of aluminum in their diet daily. Assuming 0.1% bioavailability, this is 0.01mg per day. Over a year, that's equivalent to a 4mg injection of aluminum. So more than you get from the entire vaccine schedule.
Edit: I forgot children were tiny. Whoops. So you still get more AL in your blood from the vaccines than normal food.
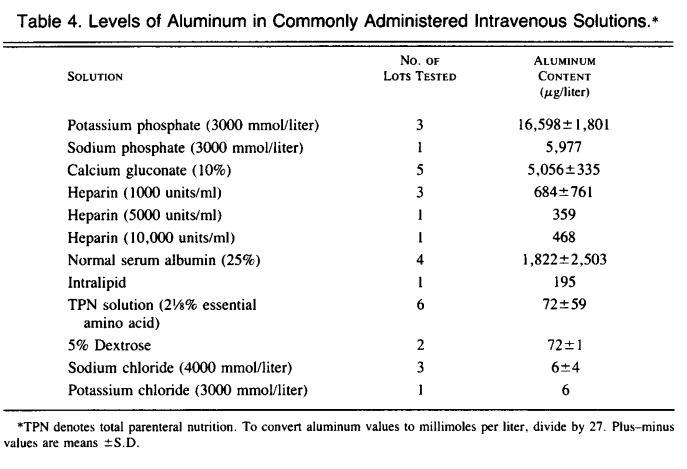
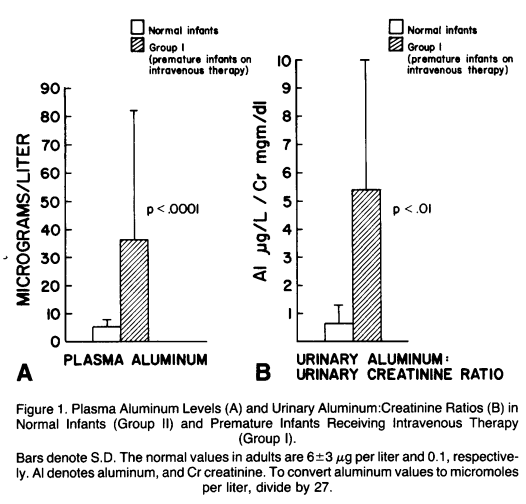
Edit2: It turns out that people actually just went and injected premature infants with massive amounts of IV aluminum until some had toxic levels of AL. Apparently, some were getting 100ug of IV AL per day, most of it from non-food IVs (16.6 mg/L for potassium, which is just nuts).
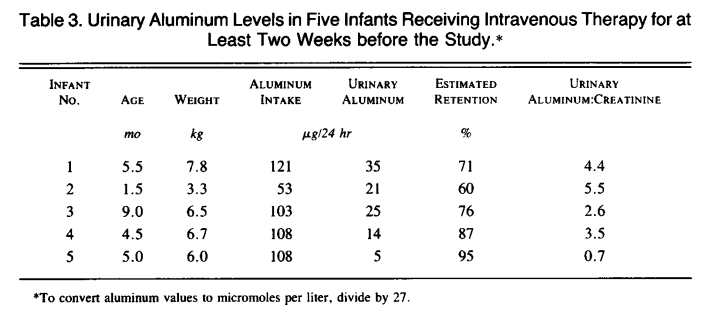
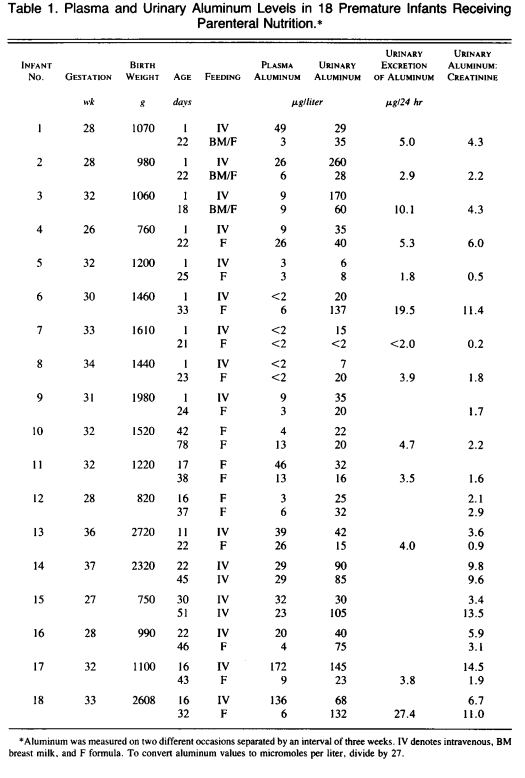
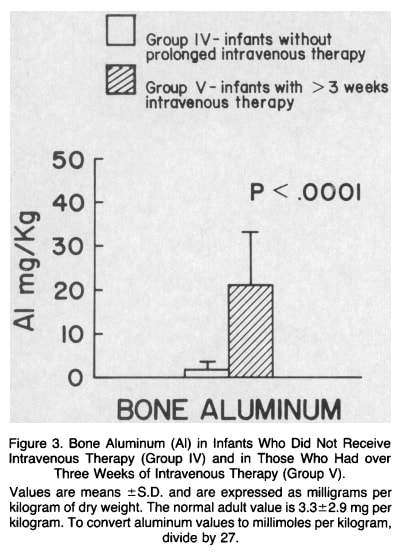
The infants in this study were injected with <3mg of IV AL over the course of a few weeks, and you see 10x levels of AL in all their tissues compared to controls. If we take ~100 ug/day, multiply that by 20 days, we get~2mg of aluminum. The highest blood AL levels detected was 172, so I guess in a worst-case scenario, for the Hep B vaccine at birth (200 ug AL), you can expect an increase of ~17 ug/L of blood AL for a few days/weeks? That seems fine? And every shot afterward is for a much bigger child, so I don't think it's too problematic. Premies also seem to have similar renal AL expulsion rates as adults most of the time. Except when they don't. I think you can maybe make a precautionary case about the at-birth Hep B vaccine specifically for renal-impaired premies, but not anything else.
And yes, it looks like the AL is sinking into the bones. A newborn has 80 g of bone on average, and 20mg/kg * 0.08kg = 1.6mg of aluminum. That's where it all went! The numbers end up working out, which is nice.
Is there maybe a way for immune cells to carry aluminum directly to the brain? Possible. If you find a paper finding evidence of that, I'll take a look at it, but my intuition is that it's unlikely.
edit 3/4: for those coming off here the front page: on further inspection from the discussions below, and after looking into Bishop's follow-up study and lack of similar follow-ups, it seems quite possible the original Bishop paper's analysis was subject to selection effects / p-hacking. But if we ignore the Bishop paper, we are still in the position of multiplying the aluminum intake of infants by a large factor, without ever having done careful studies on long-term side effects. See other threads for discussion on animal studies and neurotoxity.
edit 1: T...
Remember, aluminum can only cause brain damage if it reaches toxic levels.
What evidence do we have for the claim? Why wouldn't there be a linear relationship between the amount of aluminum in the brain and the amount of damage?
Starting a new comment chain here for the debate on immune cell transport of aluminum:
A pretty succinct argument with citations is given here, claiming that injected aluminum hydroxide is in an insoluble state above ph7.35, so immune cells capture it.
I guess after that, it's assumed they'll take it through the blood brain barrier, and drop it when / where they die? For the ones that die in the brain, and they don't need to drop very much to cause a problem, because brain Al levels are usually very low and are retained with extremely long half life.
I ...
33
I'm amazed both by the substantial lack of key evidence regarding the effectivity and safety of at least some vaccines, and by the radicalization of the discourse everywhere, even here, where you can rarely express an opinion without being heavily censored or criticised.
An example:
I gain nothing by doubting the effectivity and safety of any treatment. I don't work in the industry, I don't monetize my opinions, I don't even get social points. If I express my doubts is because I'm worried and want to know the truth. For some reason, this is politically incorrect in most circumstances.
Why and how this topic became taboo? Even if I'm stupid, and ignorant, I act in good faith, I truly want to know and, in case I'm right, to help people. Why am I censored for asking questions and showing some weak points in the narrative?
There's a difference between asking questions and making arguments where you expect other people to watch Youtube videos, especially in the comments of another thread that's not centrally about vaccination.
If you want to make a point about common beliefs about the deaths prevented by vaccines being wrong, it would make more sense to do that as a top-level post and lay out the full argument so that it's not necessary to watch any external websites to judge the argument.
I searched on lesswrong for "vaccine aluminum" and found a guy complaining about these same issues 8 years ago. Seems we sent their comments to the shadow realm
30
This reminds me of when I found an error in a popular asteroid impact effects calculator. The calculator suggested that an impact would generate only very minor earthquakes. For instance, if the Moon were to collide with the Earth, it would barely be noticeable on the other side of the planet.
I reached out to the creator of this model. They responded by explaining that their data is derived from a study on the effects of minor impacts on the Moon, as measured by a certain Apollo scientific instrument.
The study concluded that minor impactors contribute less than 0.0001% of their energy to seismic waves. However, I believe there is a significant difference between minor impactors on the Moon and larger impactors on Earth. Minor impactors hit a solid surface, and most of their kinetic energy is directed into ricocheting debris, with only a tiny fraction becoming sound waves.
In contrast, larger (kilometer-sized) impactors on Earth would penetrate deep underground, and the Earth's surface around them would behave more like a liquid. This liquid-like surface would create a large 'splash', and a significant portion of the impact energy would be converted into waves—I estimate this to be between 1 and 10 percent.
Consequently, I believe that the seismic effects of potential impactors are underestimated when compared to more widely-recognized effects such as global tsunamis and climate change.
10
If you want to read more about the science behind aluminium adjuvants, http://vaccinepapers.org/ is a goldmine of info mainly about aluminium in vaccines.
http://vaccinepapers.org/the-foundation-for-al-adjuvant-safety-is-false/ is also worth a read.
TLDR: the science behind the safety of aluminium adjuvants is sorely lacking.
10
Here is another study that seems relevant:
https://pubmed.ncbi.nlm.nih.gov/22001122/
Aluminum is a ubiquitous element that is released naturally into the environment via volcanic activity and the breakdown of rocks on the earth's surface. Exposure of the general population to aluminum occurs primarily through the consumption of food, antacids, and buffered analgesics. Exposure to aluminum in the general population can also occur through vaccination, since vaccines often contain aluminum salts (frequently aluminum hydroxide or aluminum phosphate) as adjuvants. Because concerns have been expressed by the public that aluminum in vaccines may pose a risk to infants, we developed an up-to-date analysis of the safety of aluminum adjuvants. Keith et al. [1] previously analyzed the pharmacokinetics of aluminum for infant dietary and vaccine exposures and compared the resulting body burdens to those based on the minimal risk levels (MRLs) established by the Agency for Toxic Substances and Disease Registry. We updated the analysis of Keith et al. [1] with a current pediatric vaccination schedule [2]; baseline aluminum levels at birth; an aluminum retention function that reflects changing glomerular filtration rates in infants; an adjustment for the kinetics of aluminum efflux at the site of injection; contemporaneous MRLs; and the most recent infant body weight data for children 0-60 months of age [3]. Using these updated parameters we found that the body burden of aluminum from vaccines and diet throughout an infant's first year of life is significantly less than the corresponding safe body burden of aluminum modeled using the regulatory MRL. We conclude that episodic exposures to vaccines that contain aluminum adjuvant continue to be extremely low risk to infants and that the benefits of using vaccines containing aluminum adjuvant outweigh any theoretical concerns.
*
-52-Alternatives to aluminum exist, including mRNA and other new adjuvants.
This is not really true. Despite aluminium being a neurotoxin that is detrimental at any dose just like mercury, with identical neurotoxic effects as mercury, no viable alternatives exist that were as extensively tested, and most alternatives are in fact much more dangerous. I'm not an expert on mRNA, but we have all seen with the covid shots that the side-effects were much more extreme. And for all we know it didn't need adjuvants because the spike protein itself is cytotoxic.
This is not to say that we can't develop better adjuvants, for example by using natural chemokines, which are of course not licensable hence not researched. However, this would only really address the small subset of the population, who are sensitive to heavy metals and somehow can't detoxify from them as effectively as others. Autoimmune reactions, anaphylaxis and other side-effects of vaccines, some of them also resulting in encephalitis and subsequently autism, will still persist even with healthier adjuvants, due to the nature of artificially provoking the immune system, which sometimes just leads to unpredictable immune reactions, no matter what you do.
Conceivably you could work out some extended-release nanoparticle coating to mitigate this problem. But who cares about that, if manufacturers are exempt from liability anyway?
Of course with such a lunatic vaccine schedule as found in the US that has close to 100 shots, the toxic metal poison with longest half-life estimated around 7 years, accumulates so much that it is predestined to cause all sorts of neurological dysfunction. In a sane vaccine schedule, you have just 10 shots and the ability for people to opt out. Aluminium then isn't really a major priority to improve vaccine safety. There is even limited research and reason to believe that aluminium hydroxide does not cross the blood-brain barrier that much in most people. But of course the overall toxocology of aluminium is not that simple. Especially if you inject doses that are between 10 - 100 times higher than what you would naturally absorb through food.
Bottom line is we don't really know about adjuvant safety, because really no one cares, and no one does the studies. With a little bit more censorship and vaccine Lysenkoism, the profits are just rolling and keep on rolling. Anti-vaxxer science is fascist science that undermines society and harms the greater good. That's all you really need to know about.
I am a PhD biostatistician who has worked on a project in this area. I am hoping to crowdsource opinions on this issue, especially from readers with knowledge of neurology, nephrology and/or toxicology.

The recent news cycle motivated me to spend some time reading up on the safety literature for aluminum vaccines. Aluminum is not in the Covid vaccine, but it is in many childhood vaccines.
I am deeply unsettled by what I found. Here is a summary. I would appreciate being corrected in the comments:
- The science on this topic is surprisingly neglected. Aluminum is a known neurotoxin in small concentrations in the brain. So, the obvious follow-up question: "Is the amount accumulated from childhood vaccines so small as to be irrelevant?" Unfortunately, aluminum has not undergone rigorous safety testing for cumulative cognitive effects. The fact that I could not find a convincing answer reflects a multi-decade policy failure.
-The evidence for safety cited by regulators and mainstream review papers appears to have gaping issues (see end of post for notes on the studies Mitkus et al (2011) and Karwowski et al (2018). They do not justify anywhere near the amount of faith being placed in them.)
-Mainstream educational sources are gaslighting readers by suggesting that the net exposure in vaccines is less than dietary exposure, e.g. here is what CHOP's Vaccine Education Research Center says
but this fails sanity checks with basic multiplication, given the oral bioavailability of aluminum is about 0.1 - 0.3% in diet and <0.01% in antacids according to the ATSDR. No wonder people are going nuts about the public health experts.
-There is a whole literature of claims on blood brain barrier mechanics, chemical state of the aluminum after injection, and transport via macrophages, which regulators are ignoring, but should probably affect the analysis of Mitkus 2011. I am entirely unqualified to judge and don't particularly trust this literature, so I'm ignoring this but looking forward to comments on the topic.
-Alternatives to aluminum exist, including mRNA and other new adjuvants. In the 2000's, regulators pushed industry to remove mercury from childhood vaccines; they should consider doing this again.
-A cognitive tax due to aluminum on the scale of ~0.1 IQ point for the first Hepatitis B shot is plausible (that's just from the first 250 micrograms of Al. There are > 4 mg in the whole schedule). That's my rough fermi estimate, based on an experiment showing developmental delay in premature infants exposed to hundreds of micrograms aluminum in IV fluids (Bishop et al 1997). This estimate is extremely sensitive to assumptions about renal clearance and sensitivity of brain development in premature infants compared to full term. Can anyone suggest a more accurate method? With this approach: does anyone know enough nephrology to pin down the length of time that intravenous aluminum in Bishop's premies would have spent circulating in blood, given their reduced renal function? Anyone know enough neuro to comment on whether impacts on cognitive development should be linear in the amount of neurotoxin? How much larger should it be in premies vs term infants?
______
Notes on failures in the literature:
Claims of safety of aluminum seem to bottom out in mainly two papers: Karwowski et al (2018) and Mitkus et al (2011). The FDA cites Mitkus 2011 to determine a tolerable risk level of aluminum exposure and argues that vaccine exposure is below it; the UK health authority and various review papers (such as this one) cite Karwowski as evidence of low accumulation of aluminum in infants.
Study 1
-Mitkus et al (2011) which the FDA commissioned on this topic, argues that exposure to aluminum due to vaccines is low compared to oral exposure limits. The trouble is that the study uses an old and unusually large dietary absorption figure (0.78%) [apparently Keith et al 2002, to which Mitkus is an update, uses the same number], and that 0.78% number is now well out of range from more recent estimates: average 0.1% bioavailability from diet according to the ATSDR.
This criticism is also made here. If this criticism is correct, vaccine exposure appears to be well above the scale of dietary aluminum exposure. Eyeballing the figures in Mitkus, reducing the MRL by a factor of 8 seems to consume more or less the entire safety margin, and should reverse the conclusion of safety. I have been unable to find an adequate regulatory response to this criticism.
_________
Study 2:
-Karwowski et al (2018) is cited in a number of review articles to argue that the body aluminum burden in infants attributable to vaccine Al content has been minimal. But based on the limited results presented, the study does not seem capable of supporting such a takeaway, due to lack of variability in the regressor variable (total vaccine aluminum dose). The analysis runs a regression and finds that aluminum contents in the blood and hair of 9-13-month-olds are not correlated with prior vaccination aluminum exposure. But the spread of the aluminum exposure range in their data is incredibly small, so this regression analysis could not have had any power to detect a signal. I can't be certain because they don't plot their data or report a coefficient table, but the paper says of their sample: "Median estimated cumulative vaccine aluminum load was 2.9 mg (range: 1.43-3.55mg, IQR = 0.11mg)." Most of their patients were following the schedule - great for the patients! But terrible for the experiment quality. The small variability they did have was probably age-correlated - so, the increased aluminum due to having had more shots would have been spread out in a larger infant's body. Not to mention, hair gets cut by the time a child reaches 13 months, blood clears rapidly, and the early exposure is probably what matters most for the brain. This study appears to be basically useless, and it is damning that a mainstream review such as Destafano, Bodenstab, and Offit (2019) would say: "The strongest evidence of the safety of aluminum in childhood vaccines is provided by [Karwowski et al 2018]."