5 Answers sorted by
*
930Changelog:
- 23 July 2022
- Public Health Emergency of International Concern declared.
- 25 June 2022.
- Global spread determined. Monkeypox has 10+ confirmed cases in non-endemic countries totaling over 15% of world population and GDP.
- Asymptomatic or low-symptomatic spread determined. Monkeypox sometimes leaves scabs that are small and hard to see, and may even transmit asymptomatically.
- These changes mean that monkeypox fits 5/15 criteria.
- Forecasts for individual criteria and rough long-term modeling included. Because monkeypox seems overwhelmingly likely not to cause a global pandemic and has attained what I expect is a point of long-term stability in terms of the number of checklist criteria it fulfills, I will no longer be regularly updating this checklist.
- 17 June 2022.
- Lower CFR determined: It has been nearly a month since 100 confirmed/suspected cases were announced, and 3 weeks since 200 confirmed/suspected cases were announced. Monkeypox symptoms lasts 2-4 weeks, and there have been
zeroone death so far. Based on this, it appears that in the non-African countries affected early in the outbreak, the CFR is < 1%. This may change if the virus takes hold in less affluent non-endemic countries. EDIT: there was one death reported to the WHO but not reflected in the source I was using to write this comment. - Demographic restriction: "Most cases" (i.e. > 50%, and possibly as high as 97%) are among men who have sex with men (MSM). The MSM population is 0.03-6.5% of men among all studies. This indicates that the most heavily affected population is < 15% of the total population.
- Note: Cases continue to expand geographically, and we may very well see at least 10 confirmed/suspected cases in countries comprising 15% of world population (currently we're at 13.6%).
- Overall, the outbreak now meets 3/14 criteria, though that may increase back to 4/14 criteria with further geographic spread.
- Lower CFR determined: It has been nearly a month since 100 confirmed/suspected cases were announced, and 3 weeks since 200 confirmed/suspected cases were announced. Monkeypox symptoms lasts 2-4 weeks, and there have been
- As of 14 June 2022, I am continuing to monitor the situation and will update this post if and when new checklist criteria are met.
- 27 May 2022. With 10 confirmed cases in the USA, monkeypox has now infected at least 10 people in countries comprising 40% of world GDP and 8% of world population - not enough to meet the criteria of 15% of world GDP and population in non-endemic countries.
- 25 May 2022. Absence of any inherent geographic restriction on transmissibility changed from "unclear" to "yes," and updated information about spread of the virus across populations and economies.
6/14 criteria met so far.
I can't give you a perfect answer, but given that this is a novel illness on the front page of a major newspaper, it looks like it's time to pull out the checklist. Monkeypox currently meets 6/14 criteria for being in the approach phase for a possible pandemic. Note that many of the unmet factors are just reflective of the fact that it has not reached pandemic or proto-pandemic-level spread.
For comparison, Sars-CoV2 met 13/14 criteria by Feb. 20, 2020, about 2 months after it was first reported and just before the stock market crashed.
Qualitatively, we have effective and approved vaccine technology. Probably most importantly, despite it being over a month since we had 100 cases, nearly 4 weeks since we had 200 cases, and with over 4,000 cases now, only one person has died.
The disease (as we have seen it in the past) does not appear to may not probably does sometimes spread asymptomatically or with hard-to-detect/interpret symptoms. There is no guarantee that our vaccines will be effective against any possible changes in this monkeypox.
My interpretation is that this is a disease almost exclusively spreading within a highly promiscuous sexual network of men who have sex with men. Because this community is small, this high-infection pathway for transmission is probably contained by demography and poses little risk of spread into other demographics. Fortunately, it does not appear to be particularly life-threatening with access to modern medical care. I think this is a disease that people inside of the community most affected should treat with caution, but that those not having sex with promiscuous men who have sex with promiscuous men can probably safely ignore from a practical perspective.
Forecast from 25 June 2022:
What is the chance of this disease attaining 13/14 criteria, comparable to COVID-19? I have made some forecasts for individiual criteria. The interdependencies are complex. total deaths is dependent on CFR and infection counts. Spread to new demographics and vaccine escape are probably dependent on sheer number of cases. Hospital overwhelm, quarantines, pharmaceutical company efforts, and newspaper coverage are probably dependent on number of cases at a given time. However, under a perhaps dubious simplifying assumption that the chance of each criteria is independent, my raw Monte Carlo-based forecast is as follows:
- 5/14: 9%
- 6/14: 39%
- 7/14: 35%
- 8/14: 15%
- 9/14: 2%
- 10/14+: 0%
We can try "seeding this with uncertainty" to address the many modeling shortcomings and remaining questions. One way we can do this is by assigning each remaining serious possibility (5/14-12/14) equal probabilities of 12.5%, then addressing the "complete uncertainty" model in which all criteria could change somehow with equal probabilities of 7%, and then weighting the Monte Carlo model vs. the equal probabilities model (say a 70%/27%/3% weighted split). This gives probabilities as follows:
- 0 to 4/14: 0.8%
- 5/14: 9.5%
- 6/14: 31%
- 7/14: 28%
- 8/14: 14%
- 9/14: 5.4%
- 10/14: 3.7%
- 11/14: 3.6%
- 12/14: 3.6%
- 13 to 14/14: 0.4%
It therefore seems vanishingly unlikely that monkeypox will become comparable to COVID-19 in terms of the number of deaths or economic devastation that will be attributable to it in the long run.
Transmissibility: efficiency, intra-community spread, inter-community spread, outside view
- Is there an efficient transmission route, such as respiratory droplets, airborne transmission or via the bites of common jumping or flying insects? Yes.
- "It can also spread from person to person through respiratory droplets, typically in a close setting, according to the CDC."
- Does it seem to spread rapidly within affected communities, going from a few cases to a major local emergency within a month? If R0 has been credibly estimated, is the mean of the range higher than 1? Yes.
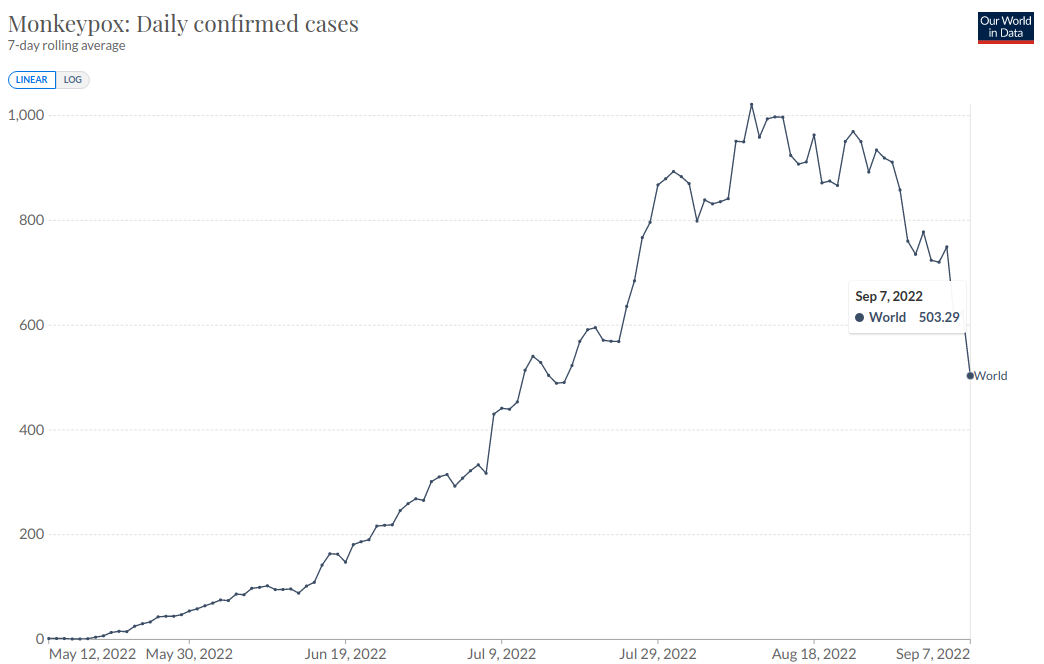
- Spain nearly doubled its cases over 9 days, increasing from 584 on 15 June 2022 to 1006 confirmed cases on 24 June 2022. The USA also doubled its cases over 9 days, going from 99 confirmed cases to 201 over the same time period.
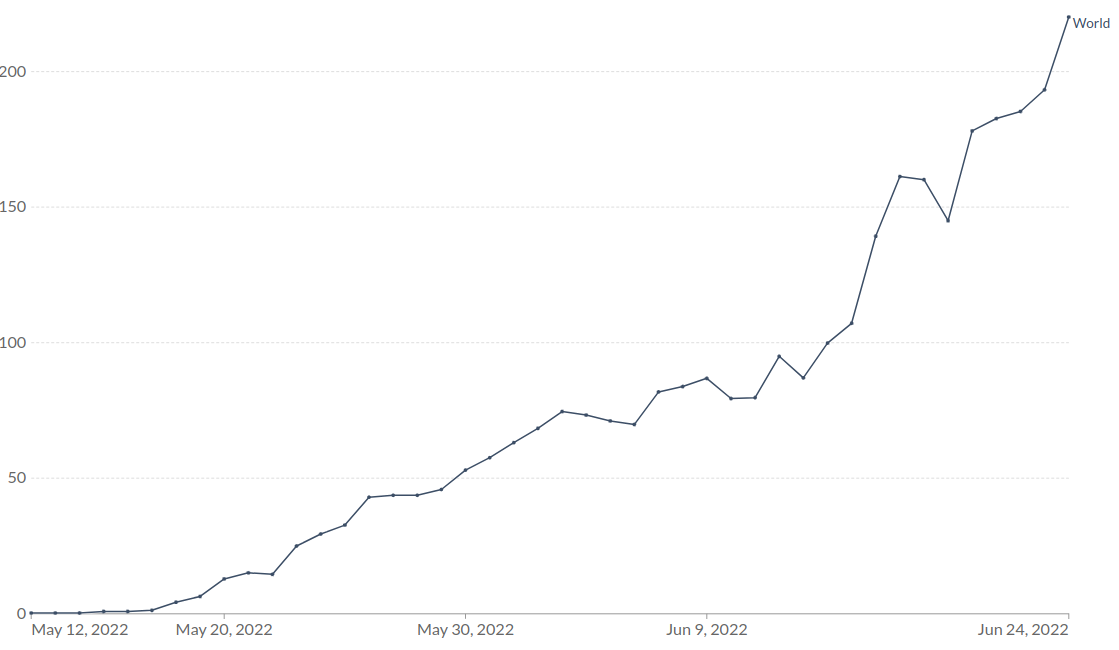 - Our World In Data, Monkeypox: Daily confirmed cases, by date of confirmation, 7-day rolling average, 24 June 2022
- Our World In Data, Monkeypox: Daily confirmed cases, by date of confirmation, 7-day rolling average, 24 June 2022- "The CDC says it is also tracking multiple clusters of monkeypox that have been reported within the past two weeks in several countries that don't normally report monkeypox, including Portugal, Spain, and the United Kingdom."
- "We do have a level of concern that this is very different than what we typically think of from monkeypox." - Jennifer McQuiston, CDC
- Has it achieved community spread in non-endemic countries on at least 3 continents, and in a set of countries comprising 15% of the world population (excluding endemic countries) and a total of 15% of world GDP? Yes (data).
- CDC defines "community spread" as "people have been infected with the virus in an area, including some who are not sure how or where they became infected," but this is not a universal definition and hard to determine from the news. I will use "at least 10 confirmed or suspected cases" as the criterion.
- These countries comprised 16% of non-endemic world population and 52% of world GDP (excluding endemic countries) on 25 June 2022.
- Is screening for the disease difficult due to test unavailability/unreliability/slowness, vector-based transmission, or transmissibility that is highest in early/asymptomatic stages? Yes.
- A report exists from 2020 that describes asymptomatic spread in Cameroon.
- "In fact, some patients have only one or two small lesions that can easily be confused with lesions caused by several sexually transmitted diseases, such as herpes and syphilis. "I think that's actually supercritical," Vinh says, "Because you can see how these patients can be missed. But they are still contagious and may propagate the disease."... So in the classic monkeypox, described in textbooks, you're supposed to have two phases," Vinh says. But in this current outbreak, many people's symptoms don't fit this profile at all, say Vinh and several doctors involved with these cases. For starters, the rash often isn't on the face or extremities at all. Instead, it typically begins on the genitals or the anus. And sometimes it doesn't spread to other parts of the body. "You don't have head-to-toe skin pox lesions," Vinh says. "Instead it's localized to just one region of the body, like the genital regions. And some people have just one or two pox. So it's not numerous." "Sometimes it's not even a pox," he says, "but rather an ulcer or a crater."' - NPR interview with Donald Vinh, infectious disease doctor at McGill University.
- "Infection with monkeypox virus begins with an incubation period. A person is not contagious during this period... Persons with monkeypox will develop an early set of symptoms (prodrome). A person may sometimes be contagious during this period." - CDC
Danger: case fatality rates, overwhelm, economic impacts, treatment
- If a credible case fatality rate has been estimated, is it 1% or higher? Alternatively, is the number of deaths divided by the number of confirmed cases being reported at around 5% or higher in at least 3 countries with reliable data? No.
- 23 July 2022: Over 17,000 cases have occurred, and the 5 reported deaths have occurred exclusively in African countries. This strongly indicates that the CFR is far below 1% outside of Africa.
- Is there a concern about hospital overwhelm or medical supply shortages in industrialized nations? No.
- This disease requires isolation of the infected person. I suspect a 10% chance of widespread overwhelm and shortages if it stays constrained to the MSM population (80%) or an 80% chance of a period of overwhelm and shortages should it escape (20%). Total probability: 24%.
- Does the disease heavily affect career-age people (age 25-65), or frequently leave survivors with lasting disability? No.
- "The case fatality ratio of monkeypox has varied between 0 and 11 % in the general population, and has been higher among young children. In addition, persons younger than 40 or 50 years of age (depending on the country) may be more susceptible to monkeypox as a result of the termination of routine smallpox vaccination worldwide after the eradication of smallpox." - WHO
- "Severe cases occur more commonly among children and are related to the extent of virus exposure, patient health status and nature of complications. Complications of monkeypox can include secondary infections, bronchopneumonia, sepsis, encephalitis, and infection of the cornea with ensuing loss of vision."
- Is there no clearly effective treatment or vaccine? No.
- "Vaccination against smallpox with vaccinia vaccine was demonstrated through several observational studies to be about 85% effective in preventing monkeypox."
- "However at the present time, the original (first-generation) smallpox vaccines are no longer available to the general public. A newer vaccinia-based vaccine was approved for the prevention of smallpox and monkeypox in 2019 and is also not yet widely available in the public sector."
- "There is currently no specific treatment recommended for monkeypox."
- Will the vaccines lose their efficacy if the virus mutates? Given that it's not too infectious and the ring vaccination strategy, I don't think this is the primary factor the virus is being selected against. My prediction is that there's a 10% chance this happens, contingent on my 80% probability that the virus remains primarily constrained to the MSM population. If it escapes into the broader population, then I'd give an 80% chance this will happen. I'll predict a total probability of this happening at 24%.
Spread limitations: demographics, geography
- If some non-age-related demographics are heavily affected and others are not, do the heavily affected demographics amount to 15% or more of the population? If almost the whole population is about equally affected, mark this criteria as met. No.
- "Most cases are in men who have sex with men" - CIDRAP
- How many is "most?" I don't have a hard number for that, but > 340 in 350 cases were among men (but not necessarily MSM) as of 28 May 2022. - Bisanzio, D., & Reithinger, R. (2022).
- Men who have sex with men accounted for 0.03% to 6.5% of men among all studies and ranged from 3.8% to 6.4% in the US, 7,000 to 39,100 in Canada, 0.03% to 6.5% in European countries, and 127,947 to 182,624 in Australia. - Mauck, Daniel E., et al. (2019)
- It's important to ask whether this will change. Will monkeypox jump outside of the MSM population? My prediction: 20% chance this will happen.
- "Most cases are in men who have sex with men" - CIDRAP
- Is the disease potentially transmissible across most of the world population (i.e. does not work via a vector that has a geographically limited range)? Yes.
- "Monkeypox virus is mostly transmitted to people from wild animals such as rodents and primates, but human-to-human transmission also occurs." - WHO
- The ability of the virus to spread across the world during this outbreak convinces me to mark this item "yes."
Social effects: communications, shutdown, research, deaths
- Has the disease made front page news on at least 3 different days in the New York Times, and also received the WHO designation "public health emergency of international concern" or the equivalent? Yes.
- My prediction: 15% chance this will happen. [Note: this prediction was incorrect and very overconfident.]
- Has there been a quarantine of a city with over 1 million inhabitants? In a country comprising at least 5% of world population or GDP, has there been a cancellation of major public events, or travel restrictions on passengers arriving from or via this country? No.
- My prediction: 3% chance this will happen.
- Has the pharmaceutical industry begun a widespread research effort to produce a novel treatment or novel vaccine, and/or has industry begun a major emergency effort to build physical infrastructure or equipment (hospitals, ventilators, etc)? No.
- My prediction: 3% chance this will happen.
- Have the death toll reached at least 2,000? No.
- "As of 15 June, a total of 2103 laboratory confirmed cases and one probable case, including one death, have been reported to WHO." - WHO
- My prediction: 75% chance this will happen - let's say by 2030.
- Let's do a Fermi estimate by comparison with HIV, another disease spreading heavily through sexual contact via MSM. Cases of MSM with HIV total about 0.1% of the US population. If monkeypox attains community spread in countries totaling 25% of world population, and infects 0.1% of the population of these countries, that is about 2 million people potentially infected.
- There is also still a chance that the social response will contain viral spread, perhaps constraining it by 1-2 OOMs. I actually assign a higher probability that it constrains monkeypox by 2 OOMs than 1 OOM due to the nature of exponential growth. Let's estimate a 25% chance of constraint to 20,000 cases, and a 75% chance of no constraint.
- To have less than 2,000 deaths, a CFR of < 0.1% would be required if there are 2 million cases, but would need to be < 10% if there are 20,000 cases. It's clear that the CFR is much less than 10%. More than 1,000 cases of monkeypox were reported to WHO on 8 June 2022, 17 days ago, and 2,000 cases were reported as of 15 June 2022, 10 days ago. There has been one death so far. The challenge is knowing when that person was infected. Worst case scenario is probably a CFR of 1%, but it could also be closer to 0.1%. I suspect it's not much lower than 0.1%. This suggests a 75% chance that there are > 2,000 deaths, contingent on failure to constrain monkeypox to below 100,000 infections or so.
Great info, thanks!
I note that this particular checklist results in an alarm bell which basically cannot go off until a pandemic is already well under way. Like, the "3 continents" item or the "medical supply shortages" or "quarantine of a city" or "front page news" are essentially hindsight indicators; by that point the pandemic has already reached significant scale. In hindsight, February 20 2020 was very late to start paying attention to covid.
Why would a country share of global GDP have anything to do with a disease being on trace to become pandemic ? Do you think 10 000 000 cases in India are intrinsically less worrying than 1 000 000 in China ? Or 200 000 in the USA ?
I was gonna comment somewhere on this page "Too long, didn't read, what options should I buy?", but now we have a checklist for that. Thanks!
“Does the disease heavily affect career-age people (age 25-65), or frequently leave survivors with lasting disability?”
This is rightly ticked off as “No”, but I think it morally counts as “Yes” if there is more danger to young children. That’s scarier in itself, and from COVID it seems people are also more likely to accept very extreme NPIs to protect children, meaning there might well be a large economic impact.
210
One possible frame from which to examine the question is "Since we have no functioning public system that competently fights infectious diseases, is this a reason to short the stock market and stockpile food and so on?"
This frame is just looking mostly at a biological entity as a biological entitiy. If "sweeping through our population unresisted" is biologically what it would naturally do (since it probably will be unresisted) then... it might do that?
But if not, not. It depends on the biology the epidemiology and also maybe the responses from institutions to try to predict that. I'm pretty blackpilled on institutions at this point, but maybe we'll get lucky and the disease itself will not have the oomph within itself to actually hurt the herd?
So given its positively known biological capacities, and currently not have strong evidence that this is decisively what's going to happen.
Thus, I'm not gonna short the stock markets yet (and so on). Not for now anyway? I'm not yet allocating many resources to it myself, so my own answer practical here so far is like: "No, don't start prepping... (yet)?"
Another possible frame is: "Imagining that one is setting policy for a hypothetical competent public health system that generically prevents all reasonably possible very bad infectious diseases (aiming to eradicate many of them, of course), by always taking preventive actions that would stop every disease (based on each one's worst possible disease properties that have not been ruled out), so that by following the policy it would be the case that no actual disease ever got through, but also the system didn't waste a lot of money achieving this outcome... in that case, have observables been in fact observed that should trigger some of these generic policies?"
Applying this filter, over my personal state of knowledge, right now, for this second question, the result I get is:
YES, if a competent public health system existed with my current beliefs (which include huge error bars, and highly limited data right now) then a hypothetically competent public health system would already be acting very fast right now.
Note that I'm not in charge of US Public Medicine (yet?) and if I was then it would be responsible to learn a lot more, very fast, and then use that knowledge to make a detailed and positive case for why action or worry is not justified. I would be pulling all-nighters based on this if I had that responsibility, but I don't, so I'm not.
Instead I'm just going to drop a few bits of evidence that seem relevant to me.
Question #1: Is the disease horrifically shitty?
Answer #1: Yes. It has some body horror (with pustules and scars and stuff) and a mortality of probably ~1%. Higher mortality in children. This mostly from priors about monkeypox, which we know about from decades of study. (It could be a mortality rate of 0.1% all in by the end, but it also could be 2%. If you get it, and you're still alive 5 weeks after symptom onset, I think... maybe you lived? This means it could take 5 weeks to get a good idea of the mortality rate for really real.)
Question #2: How does it transmit?
Answer #2: Assume aerosol. Versions of monkeypox can transmit by aerosol, and so everyone working with it (running quarantines, doing medical care, etc) should make that assumption and wear anti-aerosol PPE like they were dealing with measles or covid. This might change with more data.
Question #3: Versions of it? What about THIS version?
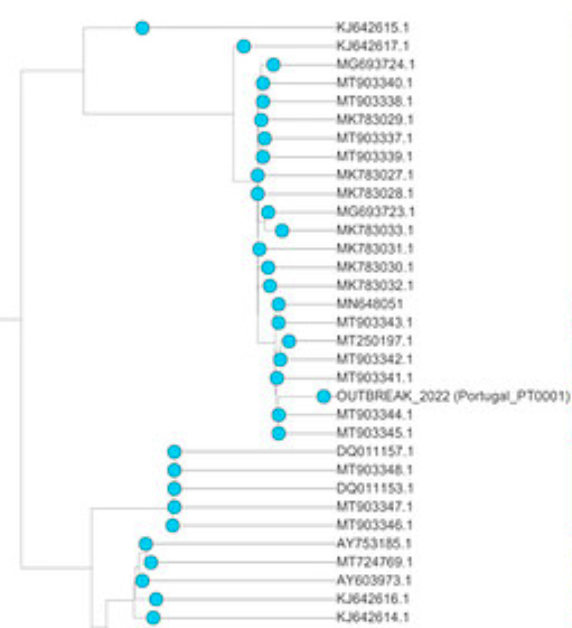
Answer #3: I was going to say that maybe no one has sequenced this thing yet... but then my google-fu kicked in, and more searching turned up a preliminary sequencing report for a draft genome that has 92% coverage, and enough data to align against known strains.
This one falls clearly among "the versions with mortality more like 1%" and is not similar to "the example with a 10% mortality" so that's nice.
That said, it has more SNPs of edit distance away from the normal ones than might be expected? So maybe it has some tricks up its sleeve that are worthy of study? Looking at the phylogentic tree built using the draft sequence (see paper linked above for details and full image, this is a zoom in), OUTBREAK_2022 clearly clusters with other light blues (that is: the west africa strain with lower mortality) BUT is farthest to the right because it has the most mutations.
Question #4: Is the R0 greater than 1?
Answer #4: Probably yes. Looking at the situation in Spain suggests GROWTH inside of localized communities. This article seems to be gleaning numbers from relatively direct reports that include: a sense of time, with few early patients, and then, later in time, more patients.
Quotes that give this suggestion include Portugal:
Portugal has confirmed the presence of the virus in five patients and has another 20 under study
Madrid:
The Community of Madrid, for its part, has put the number of patients whose symptoms suggest that they have contracted the disease at 22 , in addition to the seven already confirmed by PCR.
Then a geographic distribution that suggests that travel is occurring, with bigger (earlier seeded?) places away from the capital having more than smaller (later seeded?) places:
Four hospital sources consulted by EL PAÍS raise the number of patients treated in the last two days in hospitals in the region to "between 40 and 50". There are 16 patients from the Clinical Hospital pending confirmation of results, a dozen from the Twelve of October and several cases in the Gregorio Marañón, Ramón y Cajal and Fundación Jiménez Díaz hospitals.
These are enough OBSERVATIONS to allow me to infer a mechanistic process (of a really icky disease) that was able to generate viable human-to-human transmission via exponential growth.
Does the R0=1.1 here, or does R0=3?
I have no idea.
In the absence of knowing, it it correct policy (facing a possible exponentially growing monster that is currently small and weak but which might become large and strong in naively surprising ways to people who don't know what an exponential function is) to assume the number is higher until competently and swiftly determined to be lower and less worrisome.
But even R0=1.1 is worrisome.
The correct policy is to CAUSE the number be LOWER (if active causation is needed to achieve this), like R0=0.8 or even less than that, and then persist in that policy until the number of cases is zero... otherwise you're just dragging out the big sadness (all the individual, ad hoc, confused coping of many individuals, damaging the economy, while trapped in the fog of a hypothetically avoidable battle against mere biology) over a longer period of time.
The costs of ad hoc individual avoidance is where the huge costs pile up on the members of the public who Public Medicine officials have a duty to serve (in Lawful Good countries, anyway).
The US I think is maybe currently Chaotic Neutral? The US seems to mostly not believe in policies or causation anymore? Or to generally give a fuck, because the bureaucrats are immune from voter backlash and hold the voters in contempt and basically seem to lie to us by default while being incapable of reasoning about object level mechanisms, risks, costs, benefits, etc... For now?
I kind of hope that the 2022 and 2024 election cycles deliver new leaders who win on infectious disease policy and then clean things up... but that doesn't necessarily help us until 2023 or 2025.
Question #5: Can we effectively test for it?
Answer #5: I don't know. Everything I've heard so far is PCR testing of obviously symptomatic people, which has all kinds of slowness built into it.
I'm not sure what body compartments contain the virus and how far into the incubation period one has to get before various tests work on it.
If there are no tests, and no knowledge of test/incubation interactions then the only way TO BE SURE to prevent it from getting into a country and spreading in the community would be to shut down air travel from infected countries to my country.
Absent more detailed information, and going just from "a horrific infectious disease with R0>1 has started showing up among international travelers" I would be shutting down flights from infected countries, and putting the burden of proof on individual travelers to show positively that they are not infected during the "early confusion" period.
A fully adequate thing is probably to have people test before the flight, get diverted to a 40 quarantine after the flight, and then test out of quarantine (with positive tests diverting to isolated medical care).
I have LOOKED and almost every virus has a shorter maximum incubation period than 40 days, so that would probably be adequate, unless dealing with a bioweapon or something that was someone designed to stretch out the incubation for the sake of making it harder to detect or stop or be sure.
If you don't want to put up with 40 days in quarantine... maybe you shouldn't be flying anywhere you can't drive at the possible beginning of a possibly terrible pandemic?
Covid was handled poorly in MANY ways. One of the ways it was handled poorly is that quarantines were 14 days long despite early evidence of 27 day incubation in some cases.
Summarizing:
This won't necessarily destroy the planet or even hurt that many people. Maybe 1000 total infections ever in the world and then somehow just... done? One can hope.
Don't personally worry about it IRL yet, probably?
But also another biological disaster is not RULED OUT by the things I know, and therefore I would personally be freaking the fuck out out if I worked at the CDC and it was my responsibility to respond to deal every similar potential problem with systematically adequate levels of caution to generate systematically acceptable outcomes over all similar categories of initially observable risk.
Obviously sane things to do (at a high policy level) include:
It probably costs little to start vaccinating critical people right now with "best bet" vaccines, including people in the transporation and medical industries.
Starting challenge trials with all the known plausible vaccines against this specific disease, plus quite a few control patients (assuming informed consent and high pay) with exposure and no vaccine, with daily testing and so on, to figure out which vaccines might be perfect, and how soon people test positive if they are going to test positive.
This is PROBABLY an OVERREACTION. However the whole point of having the capacity for abstract mechanistic reasoning in service of "getting good outcomes in the world using science and policies and stuff" is that you do cheap efficient "correct" overreactions every time, and it only costs millions to overreact on the little stuff, but it saves trillions of dollars to avoid the really bad pandemics, and therefore DOING IT RIGHT EVERY TIME probably comes out "worth it on average".
I agree that this is probably an overreaction.
I don't think challenge trials are warranted. There's real harm arising from doing challenge trials. They made sense for Covid because hundreds of millions of people caught it, thousands were dying every day, and getting an effective vaccine or treatment just one day sooner could save thousands of lives. So accepting a level of harm during testing is warranted. For a disease where R seems to be not much above 1, but CFR might be as high as 10%, I would say, even if we had a competent and well-funded pandemic prevention authority, they might pass on the challenge trials this time around.
50
Has anyone done any research that human connection density due to population growth, increased travel and crowded work areas has reached a tipping point? Should multiple pandemics simply be the result of global population and superspreading in practise crossing a tipping point ?
I am not optimistic.
I think the take up of vaccines for Smallpox will be high despite serious side effects. I have seen the severity of small pox scars in survivors in my grandparents' generation. Even with a low case fatality rate of 1% the fear of facial disfigurement will push people to take the vaccine.
30
My heuristic about this is that the public is currently oversensitive on zoonotic viruses - so I feel free to not following this one until there is some more serious info.
30
One thing to remember though is that disease crossing the barrier between species are common and most don't become global pandemic. In fact SARS was bad but locally contained, MERS was almost nothing, and fears of the avian and swine flues were vastly overblown for example. So the right attitude should probably be cautious rather than worried - for now.
Is it a thing I should be allocating attention to?
Wikipedia tells me that human-to-human transmission of monkeypox is pretty rare/difficult. There has been some community spread recently at least in the UK, but that's been speculated to have been from sex. On the other hand, there's been a bunch of cases reported in Portugal and Spain recently as well. Is that just normal background rate being given more attention than usual by the news cycle? Or is this actually an unusually high number of cases? Most importantly, is the number of cases significant evidence of increased human-to-human transmission?