I also am skeptical that this effect could fail to partly fade with time or as symptoms fully go away, whereas they are claiming to not see such effects.
I'm also skeptical because effects from time in ICU for other respiratory diseases and other conditions do partly fade if you wait long enough (e.g. 6-12 months). Trying to make sense of the supplementary figures, it seems to me that nearly all subjects did the cognitive test less than 3 months after the onset of Covid (despite what the figure actually shows). Here's the figure (downloaded from this page):
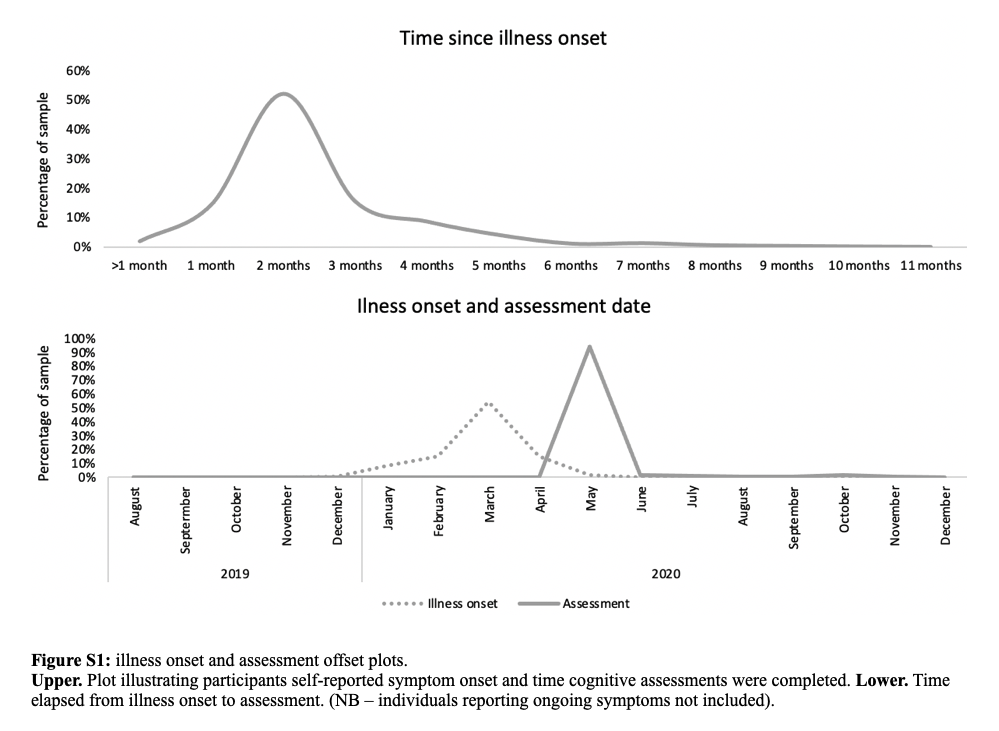
The top graph suggests a non-trivial proportion completing the assessment 3 months after onset. However, this is self-report and lots of people erroneously believed they had Covid in the early days of the epidemic (when there was almost zero testing in the UK for mild cases). The bottom graph suggests that the cognitive assessment is mostly over by the end of May. So people with onset >3 months earlier had Covid before the start of March. Yet the UK had very few cases before March: the first wave peak was after April 15. On March 13, there had been a total 10 deaths (corresponding to 1000 cases on a 1% IFR). So I think their inferred "illness onset" plot on the bottom graph is seriously flawed. I haven't run the numbers, but I'm guessing that the time from onset of Covid to assessment is (i) a narrower distribution than the top figure (due to truncating at 3 months), and (ii) has a mode shifted left of 2 months.
If I'm right in my analysis, this suggests the following:
1. The researchers were sloppy.
2. The study cannot tell us that much about Long Covid because the time since onset is too short.
Have you looked seriously into the blood clot question? I may have missed a more detailed account of your position, but my perception over the past several months has been that you're conflating 'this is not worth worrying about in the present context' with 'this is not a real effect', and that you may have justified grounds for the first claim and not for the second.
The distinction is relevant to me, an Australian who has to choose between AZ now and Pfizer soon, and whose current risk of catching Covid is extremely low. TTS is just one consideration among many, and perhaps it is swamped by the others, but I don't think that's obvious enough to skip the step of estimating the risk and taking it into account.
The Australian authorities appear to have good grounds for considering the TTS risk from AZ to be significantly above baseline. If the risk from Pfizer is similarly elevated then it probably becomes irrelevant, but it's not clear to me that the study you linked establishes that or even provides good evidence for it. See this comment on the linked page:
This is an important study, however there are some key questions remaining. The syndrome known as vaccine-induced thrombocytopenia and thrombosis (VITT) or thrombocytopenia and thrombosis syndrome (TTS), so far attributed to ChAdOx1 vaccination, is not a general clotting and thrombocytopenia condition, but a specific immune reaction mediated by anti platelet factor 4 (PF4) auto antibodies. In Australia we have been monitoring development of this condition very closely and, so far, we have detected cases of VITT following vaccination with ChAdOx1 only and not with BNT162b2. Please note that VITT is a specific syndrome with thrombosis occurring in uncommon places (eg brain venous sinuses, splanchnic veins) and high levels of markers such as D-dimer. Since this is still a rare reaction (various estimates, but about 3 per 100,000 doses), it's likely that population-based studies are not able to detect these small increases (especially since other types of thrombocytopenia and thrombosis, unrelated to VITT, are also present). The reason for concern about VITT was its high mortality rate when it was first identified. Now that the syndrome is understood in more detail, treatment options are available and the mortality rate has decreased significantly. Whether this type of autoimmune reaction occurs with BNT162b2 is yet to be determined.
(From what I have read, I believe that the non-fatal outcomes are often quite serious. So a relatively low mortality rate, while obviously welcome, is not the whole story.)
Very much agree with this - we have adverse event data from tens of millions of vaccinations, so it seems odd to suddenly ignore that on the basis of this study (doesn't look at deaths as far as I can see, and only looks at ~400,000 AZ vaccinations, mostly in people aged over 60).
My understanding is that the larger point, apart from any comparison between the AZ and Pfizer vaccines, is the "blood clot question" seemed to ignore the general population baseline. I interpreted Zvi's point about the new study as being evidence that there's no extra risk from the vaccines above the baseline risk.
That explanation is incompatible with the finding that TTS is an order of magnitude less common after the second dose than after the first. (see e.g. https://mvec.mcri.edu.au/references/thrombosis-with-thrombocytopenia-syndrome/)
It would also require our authorities to be complete idiots, beyond the level of incompetence one could reasonably expect. Unless it has literally been paid off by Pfizer, the Australian government does not have an interest in spreading FUD about AZ; quite the opposite, because our vaccine rollout strategy relied quite heavily on AZ and has been impacted in a politically-damaging way by TTS fears.
edit: better links are https://www.tga.gov.au/periodic/covid-19-vaccine-weekly-safety-report-05-08-2021 and https://www.health.gov.au/news/atagi-update-following-weekly-covid-19-meeting-28-july-2021 .
(Please note that I'm definitely not trying to discourage anyone from getting the vaccine; it is clearly much much better than taking one's chances with Covid. The practical relevance of this debate is specific to my situation as a cautious hermit in a place with very low prevalence and other vaccines expected to be available soon.)
Re: the Long Covid study.
1. The anecdotal reports of Long Covid often suggest periodic bouts of low performance rather than a permanent decline. So doing a short intelligence test is not great for measuring this. (It might still be the best thing we have).
2. We might expect smaller impact on cognition and better recovery in younger, healthier people. Do they break down further by age? Looks like <20% of the symptomatic Covid sample is under 30 and so a null result for under 25s is consistent.
3. Other surveys have found extremely high rates of people erroneously inferring they had Covid.
4. The mildest Covid is associated with a 0.5 point IQ difference. What does this mean in concrete terms? (In terms of SAT, I'd guess getting a single question wrong?). How does this compare to (a) doing the test in the morning vs the evening, (b) doing the test in the months after a bad cold, (c) doing the test after being on vacation for 4 weeks? Why does this matter? People who believe they had mild Covid in 2020 were probably quite scared on average (surveys show people view Covid as much more dangerous to younger people than it is and mild symptoms may precede severe symptoms) and they had to self-isolate for weeks. Many people were also not working or had some reduced work schedule.
The big mystery remains why Delta suddenly peaked and turned around, first in India, and now in the UK and the Netherlands. These turnarounds are excellent news, and I presume we will see a similar turnaround at a similar point, but what’s causing them to happen so quickly? I don’t know.
Regarding the covid situation in the Netherlands, it was a bit of a perfect storm of many things coming together.
- Dance clubs, events and such opened up with few restrictions - primarily entry proof for vaccination/false-tests
- Getting a single jab of J&J would instantly count as entry proof, and was heavily promoted for youths - it was also promoted to take it the same day / day before going clubbing as an alternative to testing.
- Delta variant appeared
- There was some fraud with the QR-code app for entry-proofs, unsure about how prevalent this was.
- Opening up of clubbing and such happened *before* it was even possibly for any substantial part of the 15-30 year olds to have gotten the vaccine the "regular way" at time.
Closing clubs has stopped the wave, and now a month later the majority of youths are vaccinated. And clubs are still closed. Hospital/IC admissions are now starting to go up as the initial wave has spread to mostly leftover unvaccinated 50+ year olds (I'd imagine (grand)parents of youth that went clubbing).
What follows is an outline of what happened time by time and some sources.
General positive test timing data: [1]
- Lowest point around 27-29th June
- Big inflection point up around 5th of July
- Peak already at 10th of July
A strong majority of positive tests was in ages 10-29, of which most again were in range 20-29.
Timeline of events leading up to the peak
Late June in general - Ages 20-29 that plan for the "regular" vaccine (both the RNA ones; pfizer/moderna) can start getting their first jab. This does not count as being vaccinated for things where you need vaccination-proof / false-test-proof. The second jab is late July to early August.
18th June - [2] Announcement that by the 26th of June nearly everything is open; events and such that can't be done at 1.5 meters will require vaccination/false-test proofs.
23th June - [3] 200K J&J vaccine jabs are available for taking; Youth is encouraged to get it with the slogan "Dansen met Janssen" - "Dancing with J&J". This vaccine only requires one jab so the idea was that it would be easier to get a high vaccination rate under youths using it; you only have to go out of your way once and you're done. A quick easy way to be "covid proof" for when dance clubs, festivals and holidays would open up in the weeks after it, without having to wait 6 weeks or such for a 2nd jab before it officially counts. Phone lines were absolutely swamped by demand. Would save a lot of testing for people who want to go out clubbing every weekend.
24th June - [4] CoronaCheck app updated; being vaccinated counts via this app as entry proof for events. It counts immediately after getting the vaccine, no delay.
(weekend 1; 26th, 27th of June)
26th June - [5] 175K extra J&J vaccines. Everything opens up. About the lowest point in positive test cases.
26th June - [8] At one club that was open on this very first "freedom night", 195/600 youths have tested positive in the following days.
28th June - [9] Reports on "CoronaCheck fraud"; there's a 'print' functionality for the QR-code, which makes one that doesn't time out after a few minutes. Send it to all your mates, they show it at the door. Many clubs aren't going to do the manual secondary ID card check to see if it matches, as that's frustrating customers and it already shows as "safe".
(weekend 2; 3rd, 4th of July)
6th July - [6] A mistake was corrected - Being vaccinated doesn't count as entry proof for the first 2 weeks after vaccination.
10th July - Peak day - [7] New covid rules; Dance/night clubs closed, live entertainment in catering banned, large multi-day festivals get cancelled; work at home if possible.
Vaccination related data;
[10] Official sources say that for 81% of positive tests between the 1st & 27th of July the vaccination status was known. Of those with known status, 11% was fully vaccinated, 16% partially, 73% not.
[11] Questioning of the majority of hospitals by a group of doctors got some results on vaccination status for covid hospital patients in the week of 12-18th July. About 75% was not vaccinated. About another 5% had a known problem that would reduce vaccination efficiency.
[12] People with "at least one jab", per age group: 20-35 is about 60%, 35-45 about 75%, 45-55 about 80%, 55+ is about 90%
Sources
[1] Official dutch covid dashboard; https://coronadashboard.rijksoverheid.nl/landelijk/positief-geteste-mensen
[2] Official gov site https://www.government.nl/latest/news/2021/06/18/netherlands-to-take-big-step-in-relaxing-measures-almost-everything-allowed-with-1-5-metre-distancing
[3] Dutch public broadcasting news https://nos.nl/collectie/13850/artikel/2386354-een-prik-honderden-keren-bellen-ggd-overweldigd-door-belangstelling-janssen-vaccin
[4] Official gov site https://www.rijksoverheid.nl/onderwerpen/coronavirus-covid-19/nieuws/2021/06/24/nu-ook-vaccinatiebewijzen-in-coronacheck-app
[5] https://www.rijksoverheid.nl/onderwerpen/coronavirus-covid-19/nieuws/2021/06/26/175.000-extra-janssen-vaccins-voor-keuzelijn
[6] https://www.rijksoverheid.nl/onderwerpen/coronavirus-covid-19/nieuws/2021/07/06/vaccinatiebewijs-wordt-twee-weken-na-volledige-vaccinatie-verstrekt
[7] https://www.rijksoverheid.nl/onderwerpen/coronavirus-covid-19/nieuws/2021/07/09/snelle-toename-besmettingen-dwingt-tot-maatregelen-in-de-zomer
[8] random news site; https://nieuws.nl/algemeen/20210729/superspreader-veroorzaakte-corona-uitbraak-in-club-aspen-valley/
[9] random news site; https://www.volkskrant.nl/nieuws-achtergrond/gesjoemel-met-coronacheck-is-niet-gewoon-even-screenshotje-delen~b1419271/
[10] Dutch CDC equivalent, official https://www.rivm.nl/nieuws/meer-ziekenhuisopnames-daling-aantal-positieve-coronatesten
[11] Public broadcasting news https://nos.nl/artikel/2391137-veruit-de-meeste-covidpatienten-in-ziekenhuis-zijn-niet-gevaccineerd
[12] https://www.rivm.nl/covid-19-vaccinatie/cijfers-vaccinatieprogramma you can get a table from the graph at the bottom
To add to this - there's also some sampling bias going on. As the club events opened up, a lot of visitors will be going to get tested regularly (every week, maybe even 2 times per weekend). After the peak day, when events were closed again, they don't get tested for entry proof anymore, so that also lowers positive test counts.
Though I think the general trend holds despite this.
The 'not a half life' graph is an IgM graph, not an IgG graph. IgG is the one produced in large amounts for long periods, IgM is always transient. When anyone is talking about half lives, they're probably talking about IgG.
The 'effectiveness drop' data from Pfizer, from what I understand, is confounded by changes in the dominant lineages infecting people over time.
Regarding the intelligence tests after COVID: Fourth, I can imagine some people that had COVID and go test themselves might actually want/expect to see some effect and end up not doing their best, to be a victim or have an excuse or something to blame for whatever.
Another point on how the test-taking sample may be biased- it's possible that those who expect that they have experienced cognitive decline are less likely to take the test as a way to avoid confronting reality.
Or they may be so fatigued and therefore behind on lots of life-admin tasks that signing up for a study is the last thing they'd consider.
Also, if there is a 0.5 IQ points loss in expectation, it seems to matter how it's distributed. Would everyone get the same effect or is it mostly no effect + some people lose 5 IQ points? The latter is arguably a lot worse because you can easily compensate for a small loss (drink extra caffeine when you need to be extra sharp) but not for a big one.
At the lefthand side, we have about 3 cases per 100k among the vaccinated and 9 among the unvaccinated, a ratio of 3:1. That’s a surprisingly small ratio.
The San Diego ratio is presumably "surprisingly small" because they're doing the dumb thing where they compare the "fully vaccinated" (defined as anyone who has had all doses of their vaccine for >=14 days) with the "not fully vaccinated" (defined as the remainder of the population, i.e. no vaccine, or partly vaccinated for any vaccine that gets multiple doses, or fully vaccinated but <14 days since final dose). Since those categories don't cleanly carve reality at its joints, the resulting 3:1 ratio isn't particularly meaningful without doing more math.
I don't know to which extent that problem affects the conclusions in the rest of that section, though.
Hi Zvi, you've got plenty of money and I'm really mean. Is it OK if I pay you in strong upvotes? Especially for that last bit, which is just kind of hilarious throughout.
The CDC's claim that vaccinated people have similar viral loads from Delta as unvaccinated people is now spreading far and wide on social media. The Washington Post obtained their internal slide deck here, with the unpublished data supporting this claim on slide 17.
Does anyone understand how to square this with various other studies from the past few months with more positive results for vaccine efficacy, serum neutralization, etc.? Or even better, does anyone have the actual source for this data? To me, this claim seems too extreme to be likely, but even my many PhD scientist friends mostly seem to be accepting this completely uncritically.
The Hill has published some more information:
The state health department identified 469 COVID-19 cases among Massachusetts residents who went to Provincetown, a popular vacation destination in Barnstable County, in the month of July, including 346 fully vaccinated people.
Some 127 COVID-19 samples from the fully vaccinated, including recipients of all three U.S.-authorized vaccines, showed a similar viral load to the samples from the 84 unvaccinated people.
The report noted that microbiological studies are needed to confirm that similarity in the viral load to determine whether fully vaccinated people can transmit the virus.
I still have the impression that this data could be systematically biased: it makes sense that the viral load would be high among identified cases, but randomized testing of the broader population is needed to understand the base rates.
Another consideration on the ratio between infections of unvaccinated vs vaccinated is the extent to which the different groups react to the current prevalence of Covid.
If vaccinated people relax more when prevalence is low but are much more cautious when prevalence is high then that would tend to make the ratio increase as witnessed.
This would make sense to me - being unvaccinated will be correlated with generally being less concerned about covid
The preprint for the article on cognitive decline due to long COVID was shared in the LessWrong Telegram group last October. I looked over it at the time and wrote down some notes, which I will reproduce here. Note I haven't looked through the final version of the article to check if things still match up.
I skimmed the article a bit, some things I noted:
- N=84,285 is the number of people who took the cognitive tests. Only 361 had a positive corona test
- In the abstract they say they controlled for age, gender, education level, income, racial-ethnic group and pre-existing medical disorders. In the main text they say they factored out age, sex, handedness, first language, education level, country of residence, occupational status and earnings... And then they did an additional analysis where they also considered pre-existing conditions.
- Some to my mind interesting statements from the discussion:
"Previous studies in hospitalised patients with respiratory disease not only demonstrate cognitive deficits, but suggest these remain for some at a 5 year follow-up. Consequently, the observation of post-infection deficits in the subgroup who were put on a ventilator was not surprising. Conversely, the deficits in cases who were not put on a ventilator, particularly those who remained at home, was unexpected. Although these deficits were on average of small scale for those who remained at home, they were more substantial for people who had received positive confirmation of COVID-19 infection."
"... we emphasise that longitudinal research, including follow-up of this cohort, is required to further confirm the cognitive impact of COVID-19 infection..."
"It also is plausible that cognitive deficits associated with COVID-19 are no different to other respiratory illnesses. The observation of significant cognitive deficit associated with positive biological verification of having had COVID-19, i.e., relative to suspected COVID-19, goes some way to mitigate this possibility."My personal conclusions and takeaways:
- most severe illnesses negatively impact cognitive performance
- it is probable that COVID has a neurological component such that the cognitive impact is worse
- the worse the symptoms, the worse the effect on cognitive performance --> effects from mild cases may be insignificant
- people with a compromised spleen are smarter than average (p>0.05) :D
Regarding the San Diego graph, could the relative decline of cases among the not-fully-vaccinated group be explained by an increasing fraction of that group being partially-vaccinated rather than fully-unvaccinated?
Typo? That should say ‘decreasing’. The percent of the not-fully-vaccinated that are partially vaxxed drops dramatically between June and July bc the first doses dropped dramatically at the end of May. I also assume that some of the fully vaxxed people were less than 2 weeks after their second vaccine when they caught covid (as opposed to when they got tested, often1-2 weeks later) but I know that doesn’t matter much.
ETA: This was a response to another comment, which seems to have been removed by the mods.
Suppose you were working to create a 'cure for cancer*'. Is it worth 'playing to win' there, when that's what's at stake?
*Or better treatments for some types, get something that works there, then try it for other things that seem like they'd work, etc.
Most of the time, it's not really worth it to play to win because there really isn't anything of substance to get out of winning.
More broadly, when is it worth it? In general?
I am confused by the quick turn-around in the UK, here are 3 scenarios I considered and why I am not convinced by either.
a) Herd immunity reached as the last peak infected (and made immune) the remaining people. Problems: Intuitively this would have to have been very targeted infection to cause such a quick turn / high change in immunity, as we have millions, 30% population [1] (10% adults [2]), without antibodies. We had a few hundred thousand infections maybe, so I would not expect stark changes in effective R from this.
b) Last peak & immunity in clusters of unvaccinated, or otherwise more-spreading ("party"), people? So similar to the above scenario but much more inhomogeneous, and if we just make the part of the population that is "driving" the pandemic (assuming such a part ot the population exists) immune that might lead to the decline. E.g. (i) in age-groups (young), or (ii) social circles of unvaccinated people (surely there is a correlation between your friends being vaccinated and you being vaccinated), which could be small enough so that the peak indeed corresponds to running out of people to infect? This should be possible to check, by (i) age-distribution or (ii) vaccination status of infected although I have not found that data
c) Could a significant decrease in testing make the cases appear to be lower? The positivity rate [3] dropped from ~ 11.8% (19th) to 9.6% (24th, most recent) while daily cases dropped 41.8k (19th) to 37.1k (24th) [4] --- the positivity rate dropped actually more than cases but the peak of testing (19th) was after the cases peak (43.5k on 21st), which confuses me, though the ratios between the respective peaks and 24th match. Testing rates went down but the data is rather noisy [7].
PS: Metaculus [6] prediction for large 3rd wave this year (>250 deaths/day) went down to 22% from ~ 40% 10 days ago.
Note: I checked the data & wrote most of this 3 days ago, might be slightly out of date now. Decline in UK seems to flatten now.
[1] https://ourworldindata.org/covid-vaccinations
[2] https://coronavirus.data.gov.uk/details/vaccinations
[3] https://ourworldindata.org/grapher/uk-covid-positivity?time=2021-02-04..latest
[4] https://ourworldindata.org/grapher/uk-daily-new-covid-cases?yScale=log&time=2021-05-11..latest
[5] https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/bulletins/coronaviruscovid19infectionsurveypilot/previousReleases
[6] https://www.metaculus.com/questions/7537/250-deathsday-in-uk-third-wave/
[7] https://coronavirus.data.gov.uk/details/testing
Intelligent people tend to be more rule abiding in general
As an aside, do you have a source for this? A quick search didn't turn up anything useful.
My intuition would be the opposite: if people are acting meta-rationally, then less intelligent people should be more rule-abiding because they know they're not smart enough to figure out when exceptions are worth it. But I don't have anything to back that up.
Stupider people get arrested more often for committing violent crimes. On the other hand, smarter people may commit more nonviolent crime and definitely get caught less frequently. ¯\(ツ)/¯
While there remains debate regarding the existence (and strength) of this relationship, there is a wider consensus that individuals with below average functioning (in particular cognitive impairments) are disproportionately represented within the prison population.
―The relationship between lower intelligence, crime and custodial outcomes: a brief literary review of a vulnerable group by James Freeman
Perhaps we have different reference classes for "less intelligent people". When I think "less intelligent people" I think about this man who bought beer while carrying an alligator.
The high-level explanation I'd give for this is that smart people make better decisions in general, and certain classes of bad decisions are also illegal. So perhaps the reason smart people follow rules more isn't that they're more inherently rule-abiding, but that they behave in more reasonable ways, and rules tend to be reasonable (obviously not always, but they're more reasonable than if they were assigned at random).
Few things warm my heart more than playing to win the game. Few things sadden me more than observing someone not playing to win the game.
Usually, that means they are playing a different game instead, whether they admit it or not, and whether or not they know it themselves. The game, from this perspective, is simply that which you are playing to win, and your revealed preferences define the game’s rules and objectives.
This week saw some excellent playing to win the game. The NFL, many parts of the government and a number of corporations began imposing vaccine mandates, hopefully causing a cascading effect. It’s at least a start. There’s a lot of ways in which we collectively are revealing ourselves not to be playing the game of ‘get people vaccinated’ let alone the game of ‘prevent Covid while minimizing costs.’ The lowest hanging fruit remains fully approving the vaccines, which we somehow still have not done.
A central question continues to be how effective the vaccines are against Delta. The Israeli claims turn out to probably be the result of basic statistical mistakes, so those scary numbers are now mostly off the table, although that still leaves us a range containing meaningfully distinct answers.
Another central question is Long Covid, for which we got some actual data, so there’s a section analyzing that.
The big mystery remains why Delta suddenly peaked and turned around, first in India, and now in the UK and the Netherlands. These turnarounds are excellent news, and I presume we will see a similar turnaround at a similar point, but what’s causing them to happen so quickly? I don’t know.
Meanwhile, the numbers got worse slightly faster than I expected. Let’s run them..
The Numbers
Predictions
Prediction from last week: 360,000 cases (+50%) and 1845 deaths (+10%)
Result: 392,000 cases (+62%) and 2042 deaths (+21%).
Prediction for next week: 610,000 cases (+55%) and 2,450 deaths (+20%).
Things got worse slightly faster than expected. I doubt things are ready to turn around, but there are signs of the control system starting to act which should accelerate, and between vaccinations and infections (most of which likely do not result in positive tests and therefore known cases) immunity is building up, so I continue to expect the pace of growth to drop off a bit. I’d be unsurprised by numbers between about +40% and +70% for cases.
Deaths
Deaths are going up slower than cases, but faster than one would have hoped. I interpret this partly as last week’s number being artificially low, and partly as the South having a problem with its most vulnerable being partly unvaccinated, and thus we see a rise focused on the South including as a share of the cases.
Things will continue to get worse until several weeks after cases turn around. The question is if we can continue to see deaths lag behind cases, as they continue to do so in the UK. My guess is we won’t do as well as some other places, especially in the South, but will still be doing better than our case counts alone would suggest.
Cases
Vaccinations
People respond to incentives. With the costs of not being vaccinated rising on all fronts, more people are making the decision to get vaccinated. The remaining people are harder to get, but efforts benefit from the growing social proof and social pressure from previous vaccinations. It also helps that previously reluctant politicians, with notably rare exceptions, are increasingly getting with the program.
Vaccination Effectiveness
This thread takes the Israeli evidence (that likely was a quite sloppy statistical error, see the next section), combines it with antibody measures, and suggests that antibody counts decay with a half life of a few months, so under this hypothesis vaccinations continue to protect you from severe symptoms and death but after five months lose half their effectiveness at protecting against infection. I hate the smugness and overconfidence here, and also based on the clinical trials and result of one dose it doesn’t make any sense that a 75% reduction in antibodies would cut protection against infection by 50%. Nor do I buy that there would be a threshold effect big enough to cause the curve she’s analyzing here.
Also, this isn’t a half-life:
Even if we take this fully seriously, it’s a steady state that we get to in 3-5 months, and the median gets to its low point after three (which is likely random variance, but the point stands that most of the effect is in place after month three). It certainly doesn’t seem anything like ‘half life of 100 days’ the next link in the thread cited, so I notice I’m confused.
I am noting such arguments here for completeness, but I do not put much weight on them. As usual, when one has a new hypothesis, one must then reconcile it with all the different data points, and alarming ‘vaccine stops working’ theories keep implying, well, that vaccines aren’t mostly working, when they obviously mostly are. You can’t both argue that we suddenly don’t think vaccines work as well against Delta, and that vaccine protections fade rapidly over time, and also that Delta is so much more infectious to begin with among the unvaccinated, because such claims combine to not be even slightly compatible with the observed data in other places.
Then on Wednesday, Pfizer came out with data that the vaccine remains effective after six months. That’s the headline. The actual data is not as encouraging:
Contrary to Pfizer, that’s quite the drop in effectiveness. The protection against death remains robust, and yes 84% is still quite good compared to what we would have asked for a year ago, but ‘remains effective’ is giving the wrong impression if this data holds up.
The other news here is that Pfizer plans to be calling for booster shots. It seems that a three dose regimen is much more effective than a two dose regimen, now that we’ve had the ability to test such things, and some places are moving to implement this already. The data here suggests that the third dose will bring things back to at least the early stage 96% effectiveness and plausibly even higher. If I am offered a third dose, I will happily accept it.
There is the concern that giving people third doses while others have not had the opportunity even for first doses is not ethical. I respect that perspective, but do not share it, and will leave it at that.
On That Israeli Data on Delta’s Effectiveness
Israeli data has been suggesting remarkably low effectiveness of vaccinations against Delta. This thread suggests this comes from… using the wrong denominator. The explanation is, the Israeli outbreak started in very highly vaccinated areas, and the effectiveness numbers came from the percentage of cases that were among the vaccinated, but they were comparing that to the overall population numbers. So, whoops.
If true, as I believe it probably is, that would explain things and be on some levels comforting, but on other levels it’s the opposite of comforting, because this is saying that the Israeli outbreaks started in highly vaccinated areas. So, whoops again.
I’m inclined to believe that such simple mistakes were happening here, because the Israeli numbers simply didn’t make any sense. They were incompatible, even with each other, let alone with what we were seeing elsewhere. And I’m definitely at the point where such stupid mistakes aren’t surprising. This one is rather stupid, but that’s the way such things seem to often go.
Delta Variant
For those who need it: Thread explaining basics of how vaccine protection interacts with spread of Delta.
CDC has reversed course on its mask mandates. Masks will be back in schools, where I’ve learned first hand and the hard way that schools feel compelled to follow the guidelines. They’re suggesting indoor vaccinated masking in ‘areas where there is a surge’ which doesn’t really make a lot of sense and will cause some confusion, but perhaps the hope is it will make intuitive sense to regular people. It’s good that when the facts change, the CDC changes its mind, at least.
There are two central facts about Delta one’s model must explain. First, the dramatic takeover of the pandemic and rise in overall cases across countries. Second, the sudden reversal of those trends in many places, including India, the UK and the Netherlands:
The Dutch numbers are down by half, the UK is not far behind.
If you zoom out, the case numbers are still large.
But the death numbers barely register:
It will take another week or two for the UK/Netherlands death numbers to peak, but this is what vaccinating the vulnerable looks like where it counts.
Here’s some data from Minnesota:
If we take this at face value (it’s not normalized sufficiently so there’s a bunch of reasons not to, but they point in various directions), it suggests about the same ratios in effectiveness for Delta between the vaccines that we saw for the older strain. Moderna’s effective dose is higher than Pfizer’s, which potentially could be responsible for that differential, although I’m still mostly inclined to treat the two as the same until we get a lot more similar data points elsewhere. Normalizing properly for exactly when vaccinations were in effect is tough, but for context Minnesota at the time had just under 30k confirmed infections since May 1.
The data below from San Diego is better normalized, and I’m going to say that this is enough non-normalized data points.
This graph is pretty bizarre when taken at face value, and I presume it shouldn’t be, and is only the county of San Diego, but still seems worth noting:
Details:
At the lefthand side, we have about 3 cases per 100k among the vaccinated and 9 among the unvaccinated, a ratio of 3:1. That’s a surprisingly small ratio.
At the end of May, cases among the vaccinated level off, but cases among the unvaccinated continue to drop until about June 10.
Then the cases among the unvaccinated shoot up, and at the end, we have 16 unvaccianted cases per 100k and 2 vaccinated cases, for an 8:1 ratio. In July, this is most definitely representing a pandemic of the unvaccinated.
The question is, why would this ratio suddenly get much bigger?
If Delta is, as everyone now fears, reducing the effectiveness of vaccinations, you’d expect the ratio to go down rather than up. Whereas this new 8:1 ratio implies a much higher effectiveness level, unless one can explain it via other factors.
One possible explanation is that early on the vaccinations went to highly vulnerable people, whereas now they’re more evenly distributed, but that would only explain contrasting March with June, not June with July, where that effect is going to be small.
Another is to claim this didn’t happen:
If we look at the ratio that had emerged before that period in early June, we do get a different picture then, but that period where the unvaccinated cases are going down but vaccinated cases went up is super weird for its own reasons, and the contrast with the left side of the graph is still clear. At a minimum, a constant ratio does not suggest any decrease in effective immunity.
A third is to say that San Diego’s numbers are quirky because someone’s are going to be quirky.
Here’s another Tweet that shows Marin County:
Looking at that, I see a ratio of just over 4:1 rather than 8:1. I don’t see a big shift to higher ratios in July, but I also don’t see a shift to lower ratios either.
I tried briefly to find similar charts or data for larger areas and it wasn’t obvious where they were. If anyone can link to one it would be appreciated. The normalizations here make the data much more useful but I’d prefer a much bigger and ideally more representative area.
Vaccinations are great, but what matters is immunity, and vaccines are only one way to get immunity. Antibodies are not a perfect proxy for immunity, but they’re likely the best one available, and the numbers in the UK on antibodies are very, very high…
When this many people have antibodies, it’s both scary that cases for a while were going up anyway, and also easy to understand how there might be a rapid peak followed by a reversal. It’s especially easy to see this if the serial interval averages two or three days instead of five, so things that happen tend to happen fast.
If 90% of people are immune, then each additional 1% that becomes immune reduces spread after that by a full 10% even if everyone is otherwise identical. Whatever vectors still remain for the virus to spread burn themselves out rapidly, until there isn’t enough left to sustain the pandemic.
It is possible that this is simply what it takes to turn the corner on Delta. If so, then if the USA has roughly 70% of adults having been vaccinated, than we would turn the corner when about two thirds of the unvaccinated have been infected at some point sufficiently to develop antibodies, with the understanding that many Covid infections don’t lead to a positive test and therefore don’t show up in the statistics, and also a lot of them already happened over the past year and a half.
It still doesn’t explain the full extent of the rapid turnarounds in India and the UK, but it helps explain it. Lag in the control system also helps, but again I notice my model remains surprised by this.
You Play to Win the Game
Last year, the NBA figured out how to do Covid testing. This year, it’s all about vaccinations, and the NFL is stepping up.
As we all know, in the NFL and also in life, You Play To Win The Game.
Winning isn’t everything, it’s the only thing.
What does it look like to play to win, when it comes to Covid-19?
It looks like this. Here’s the key operating principles.
Here’s what would trigger a forfeit:
In other words:
If your vaccinated players force us to cancel the game, we’ll try to do the best we can for everyone involved.
If your unvaccinated players force us to cancel the game, f*** you. You forfeit the game for all purposes where you want to win, the game is cancelled for all purposes where you wanted to lose, and the league will focus on ‘minimizing the financial and competitive burden’ exclusively on the other team. Not you. You’re on your own.
Oh, and regardless of vaccination status, if there’s an outbreak that cancels the game, the players on both teams don’t get paid for that game:
That’s what it looks like when you play to win.
Some NFL players are less than thrilled with this situation.
For example:
Yes, it turns out that not protecting yourself against infectious disease can put you in a position to hurt your team. Who knew?
Who else we got?
I hope someone compiles all of these together, and then continues in the sacred tradition of arranging them into a YouTube montage video set to Taylor Swift’s I Forgot That You Existed.
Good luck, Mr. Hopkins and all the rest of you, in all your future and hopefully far away endeavors.
The Pac-12 is considering following suit. It does make a lot of sense the way the commissioner George Kliavkoff put it:
Most of the Pac-12 schools have vaccine mandates in place in any case. Washington State is currently trying to figure out what to do when its coach refuses to get with that program.
We need more of that ‘can do, and if you choose not to do that’s on you that you didn’t do it’ spirit.
Others Playing To Win the Game
The good news is we are indeed seeing more of this spirit, and there seems to be momentum behind these efforts.
New York and California are requiring government workers who don’t get vaccinated to get weekly tests and wear masks indoors. New York at least is not providing a testing option for health care workers, it’s vaccination or you are (very understandably) fired. Virginia is mandating vaccinations for health workers, as is the veterans administration.
From Bloomberg’s daily newsletter:
Reports are that Biden will follow shortly with a similar rule for federal employees, if he hasn’t already by the time you read this.
Companies are now able to get in on the act:
My hope is that this effort continues and spreads, and more and more private employers will be emboldened to enact similar policies. If I was a private employer whose employees were interacting with each other in person or with customers in person, I’d hope to be more worried about what would happen if I didn’t mandate vaccination, including legal consequences, than what would happen if I did, and this transition will go a long way. As usual, we blame people via Asymmetric Justice for action but not inaction, so the less a (soft via testing and masking requirements) mandate seems like a bold choice to take action and more like a default state that protects the employer from liability or an outbreak among the other employees, the better. These things matter.
And once again, we gotta get full authorization as soon as possible. A huge amount of the lack of mandates is the lack of full authorization. If we got it, this cascade could kick into high gear quickly, and give a justification for a change in policy. At this point, any efforts to get people vaccinated that don’t involve a demand for full authorization are impossible to take seriously. How can we be mandating vaccinations but not be ready to fully approve them?
A bonus is it creates positive selection in employees. If anyone quits or otherwise goes ballistic about the situation, that was likely a time bomb on your team in one form or another, they’re definitely bad at risk management, and this gives you the opportunity to be rid of them. It’s hard to hire right now so that could be short term trouble, but identifying and getting rid of bad employees is both highly difficult and valuable.
Many other countries also continue to get with the program. Here’s Israel this week, playing to win:
I more than fully endorse this take on all of these developments:
Long Covid
We finally have some real data to look at.
The original paper is here.
Headline findings:
This raises, and/or lets us more usefully address, multiple questions. Should we believe the results of this study? Do these effects seem real? If they are real, what can either an individual or our society in general do about this? Does this change anything if it is true?
First, no matter what the flaws here, a big thank you for running this at all. It does seem like this is a big advance in information value over previous sources. This stuff is hard, and doing something concrete is better than not doing it. This does seem to rise to the level of something useful.
Second, as usual, studying such things is really hard and there are lots of problems, so let’s get right to some of those.
First off, baseline methods.
There is an obvious concern here. People were recruited to do an intelligence test by offering them an intelligence test. Which, yes, right on, very on the nose and efficient incentivizing, but we do have to worry about the selection effects from that and whether the standard controls handle them.
Here’s what they controlled for: “Nuisance variables were age, sex, racial-ethnicity, gender, handedness, first language (English vs other), country of residence (UK vs other), education level, vocational status and annual earning.”
Handedness! So other than the bonus handedness, this is your basic check of control variables for basic demographic information and socio-economic status.
Before going further, there are three potential confounding factors here that seem like big issues.
The first is that choosing to take the test could be a function of one’s situation and practical intelligence. If I had Covid and fully recovered and felt fine, I would not be so curious about taking an intelligence test. If I had Covid and had continued problems, then I would plausibly be much more interested to know how I did on such a test. In theory, this could be the whole situation, since those who feel stupid due to non-Covid reasons or due to lockdowns wouldn’t feel the same curiosity and wouldn’t opt in, whereas those who had Covid and happened to also feel stupid recently would take the test.
The second is that being intelligent helps prevent Covid-19, after controlling for the other factors. The study was done in 2020 so vaccination isn’t relevant, but plenty of other decisions matter. How and when people decided to mask, including how much care was put into doing it properly with a good fit, determines both how likely they were to get Covid and how severe their case was likely to be. Social distancing is similar. As is making a wide variety of other good decisions about how much risk to take. Intelligence also correlates with the type of work that can be done remotely, even controlling for income and education, which improves ability to social distance. Intelligent people tend to be more rule abiding in general, including when the rule is dumb, which in this case is net useful. And so on.
The third is that it looks like they’re using self reports of Covid-19.
It makes sense to worry that people would conclude from their long term issues that they likely had Covid-19, or from a lack of such issues that they likely didn’t have it, which could once again confound the results here.
In theory, one could have controlled for all this, by having people take the test before Covid-19. Even now, one could attempt to measure the impact level of the second effect by then following up with the people who took the test and seeing which of them later got Covid, although changing conditions will change the size of the correlation – so it’s more of a ‘check if this is a substantial effect or not’ check than anything else, and now with vaccination everything is different. For the first effect, again, you’d need to find a way to measure things in the other order, possible in theory but not easy or cheap. For the third you could do antibody tests since this was pre-vaccinations.
But all of that is tricky and expensive.
The huge advantages of doing what they actually did were that it was practical, it was ‘ethical’ and it was relatively inexpensive. I point out issues, but I think the study was likely done roughly the right way in context, picking the low hanging fruit. From a civilizational perspective we could and should have done far better, but that’s not the fault of the people doing what they can.
Looking ahead, it does seem like intelligence didn’t have too big an effect on chance of getting Covid, based on a follow-up test. This could still eat up the whole observed effect, but I’m less concerned about it than before reading about that. Also a little sad that this effect turns out to be so small, for other reasons.
I also approve of their methods for analyzing the results, especially combining the nine tests into one number. There are a lot of worries I conspicuously don’t have here.
Here’s the breakdown by symptoms and gender:
I’m noting it because that righthand column is pretty strange. It’s lower average age, and suddenly it’s very male whereas the other groups are increasingly female and older as symptoms became more serious. Low sample size is presumably the answer (44 people) but it’s still kind of weird.
Lower in the same table, it’s clear that almost none of these people had a positive Covid-19 biological test, so this is almost all self-diagnosis:
Then we look at the headline chart.
One standard deviation in an IQ test is about 15 points, so this is an average of about 0.5 points or so for the first group, 1 point for those not requiring assistance, 2 for those getting help at home, 4 for those hospitalized and 7 for those who went on a ventilator.
The first thing to note is that this effect that grows as symptoms get more severe makes a hell of a lot more sense than the mysterious ‘Long Covid doesn’t care how bad your case was’ nonsense. I’m far more willing to believe a proportional effect that grows with symptoms than a blanket ‘nope, you technically got Covid and now you roll versus this other thing at constant odds’ hypothesis. And of course if you’ve been in the hospital on a respirator, it’s not going to be good for your cognitive performance.
So that adds a lot of credibility to the findings.
This is their explanation of why we shouldn’t worry about pre-morbid differences (e.g. how smart people were before):
I find this helpful but not fully convincing. One worry is that they’re claiming that those that were ill should have otherwise had higher cognitive performance. I don’t find this plausible, so it makes me skeptical their controls are sufficient. It does mean that I’m no longer concerned that the intelligence differences are too big here, since presumably Covid doesn’t help cognitive performance and that caps the differences at the effect sizes. The second check, following up with a questionnaire to see who later got Covid, is also helpful in capping the effect size of ‘smarter people get less Covid’ but doesn’t address the other concerns. I’m also sad we didn’t ask those people to retake the tests.
I also am skeptical that this effect could fail to partly fade with time or as symptoms fully go away, whereas they are claiming to not see such effects.
As always, also, there’s the question of whether this effect is unique to Covid or is a general property of many infectious diseases. In some sense it does not matter, but in other senses it matters a lot – or at least points to our failure to be consistent, with several potential ways to address that.
This is their note that the effect size here is indeed a big deal, which it is:
The line that the 0.47 SD drop is more than 10 years of decline in global performance between 20 and 70 is very interesting, because it suggests an intuitive way to measure how much we should care about this effect – we can think of this as similar to aging.
Every year, we all age one year, and a lot of stuff gets harder. For those of us over the age of 25 or so, it’s kind of terrible, and we need to put a lot more effort into making it stop.
So, in theory, this is suggesting that relatively mild (but still symptomatic) Covid is still doing something of similar magnitude to causing our brains to age two years, and as it gets more serious things get much worse. On average over all symptomatic cases we’d be looking at about three years.
If that’s all true, that’s really bad! Once again, you do not want to get Covid. And one can now think about how much life not lived would be justified in the name of not catching Covid, if one is at only small risk of death.
I don’t find it likely they are underestimating the size of this particular effect, and I can see how the effect could be smaller or not be there, so that somewhat reduces the expected effect size. But then one must also account for other distinct problems.
Then there’s the question of how this interacts with vaccinations and children. If you get long Covid roughly the same way you get other symptoms, that’s going to be a big reduction in risk, especially for the very young. My prior would be that this protection is somewhere in between the protection against infection and protection against death.
You’d also want to adjust for Delta, since all this data was from 2020. My presumption is degree of symptoms mostly controls for that, but it’s plausible that this doesn’t fully control for that.
This Long Covid effect definitely would still be a bigger danger for most people than death, even before vaccinations. I’d much rather take the very small risk of death than accept this level of accelerated cognitive decline, plus any longer term non-cognitive effects, and it isn’t close even under relatively minimizing assumptions, and multiplying for the uncertainty that this effect is real.
The question then remains, what costs are worth bearing to reduce the probability that this happens to you, individually or collectively.
Which in turn, as always, depends on one’s ability to change that number. Postponing the problem isn’t worth zero, but it’s only worth enough to care much if it buys time for a permanent solution, or there’s a permanent solution you’re willing to implement. That’s true both individually and collectively. Postponement can also help if it is ‘bending the curve’ in ways that matter, but that doesn’t impact Long Covid much.
There’s the temptation to say ‘oh no, this is terrible, something must be done, this is something, therefore we must do it’ where the something is an effort to kick a can down the road at very high cost, and which may or may not be able to do much of even that.
Vaccine Hesitancy
This LA Times piece looks at those who are getting vaccinated now in a local community, and finds highly reasonable thinking going on. Of course, these are exactly the previously hesitant people who then did get vaccinated. So it makes sense that such people would seem more reasonable, and would not be at all representative of those who still haven’t gotten their shots. It is consistent with the model that there are a bunch of people doing cost-benefit calculations who are relatively easy to get, and then a bunch of people who are much harder to get.
This thread compares anti-vax people to victims of a con, with resulting implications for how one should communicate with them if one is attempting to persuade and convince rather than make one feel better about having taken the proper symbolic action. Cooling the mark via people in the community that have earned people’s trust is so crazy an idea it just might work, but requires that such people be convinced first.
Note of course that such framing explicitly assumes the conclusion, that not only are vaccines safe and effective and the right thing for everyone both socially and individually, but that the evidence for this is so sufficient that if you don’t believe it, you’ve been conned. I don’t think that’s right. Many have effectively been conned by misinformation or the need for tribal signaling, but others are doing a calculation with different information and getting a different answer. I strongly believe they’re wrong, but it seems plausible that treating such people as con victims is (at best) highly condescending and that they would notice. We are doing a rather terrible job conveying the information about vaccines in a way that is accessible, understandable and credible to such people, and the fact that vaccines happen to be highly safe and effective doesn’t excuse that.
This paper provides an interesting model of vaccine hesitancy (via MR). In it, people are effectively doing an approximation of a cost-benefit analysis on vaccination, so the more prevalent the disease, the higher the willingness to vaccinate, which is clear from past outbreaks.
One consequence of this is that if you reduce the number of cases, vaccinations go down. Thus, this model claims vaccine passports are ‘ineffective’ in the sense that they don’t increase vaccinations, and could even backfire, because they reduce prevalence. I find their math to prove too much and therefore am confident they’re technically wrong to draw their conclusions so broadly, but accept the underlying dynamics as things that are real and that matter.
Oddly, Tyler thinks this makes a strong case against such passports. I would claim the opposite, because reducing prevalence is a good thing. If we can do something that both incentivizes vaccinations and prevents cases at the same time, that’s good, and if the reduction in cases means we don’t on net cause vaccinations, then that seems fine. Otherwise, you are in the world where you outright want more cases in order to show the bastards and own the reds, which is a bullet I really hope no one is biting.
Regardless, under such a model, lowering costs of vaccination is the obvious choice for getting people vaccinated, and it continues to be a highly efficient strategy. Drive that cost negative. More precisely, one wants to reduce perceived costs, which can involve changing people’s models of vaccine effectiveness and/or safety, and/or changing the difficulty and costs of vaccination.
Periodic Reminders (You Should Know This Already)
In case you need a short video explanation for how the mRNA vaccines work and were developed, we got you.
Your periodic reminder that our travel restrictions make absolutely zero sense (MR).
And yes, a sensible system would be entirely feasible:
This explanation rings far too true:
Your periodic reminder: The FDA and cost benefit analysis are not on speaking terms, nor does the decision process much correspond to what is safe and effective let alone what is in the public interest. Hence, we approve $50,000 drugs that don’t work and then are forced to collectively pay for them out of the public treasury, but can’t fully approve the same Covid vaccines and definitely can’t mandate them, and so on. Yeah, yeah, same old, FDA Delenda Est, stop using such procedures to tell people what they’re legally allowed to do, also stop using such procedures to decide what we pay for without looking at costs against benefits, and at a bare minimum stop equating those two decisions. The suggestion from the link of letting government officials choose what is mandatory and paid for versus what is forbidden on an ad hoc per-item basis seems to miss the point of ‘are those our only choices?’ and I’m not sure if it’s better or worse than status quo.
In other FDA Delenda Est it’s-not-news-but-it-was-news-to-him non-news:
WaPo reminds us that Japan is failing at vaccinations by doing the things you would do if you wanted to fail at vaccinations. This includes insisting on distribution by only doctors and nurses, holding out until way too late for a homegrown vaccine, a labyrinth approval process and demands for domestic testing of the vaccines, confusion about rules and a general lack of urgency, among other things.
(If for some reason you want to financially support these weekly posts and/or my writing in general, you can do so via my bare bones, no rewards of any kind Patreon that is set up exclusively for that purpose. On the margin this does shift my time a non-zero amount towards these posts. However: I do not in any way need the money, please only provide funds fully understanding I already have plenty of money, and if and to the extent that doing this would make your own life better rather than worse.)
The whole blood clot issue around AZ was never a thing. Of course Pfizer has similar instances of blood clots to AZ, given that not getting vaccinated at all also has similar instances. Also Covid-19 itself actually does cause blood clots, but hey.
The term ‘genuine’ fury is interesting here, since we knew all this already. It also does not matter, for the purposes of the EU’s motivations, whether or not the concerns turn out to be valid. Their perception of the situation at the time would remain unchanged.
Also happy to see this report properly label the people opposing AZ as anti-vaxxers, from anti meaning against and vax meaning vaccine:
To what extent is it true that the European backlash against AZ was due to spite resulting from Brexit? My guess is this was not all that central, but was a substantial contributing factor on the margin. That doesn’t especially make this better or worse, it merely notes that the European Union countries were inclined to make such a self-destructive move for overdetermined reasons.
Very Serious People do not care about physical world models, a case study (Warning: Someone Is Wrong On the Internet):
Sir, the virus did not mutate among the few remaining infections in Israel. The current pandemic in Israel is not causally related, at all, to the few remaining cases of Alpha or the original strain that were still present in Israel.
It comes from Delta. If Israel had achieved actual zero Covid but not also instituted large new measures to keep Delta out, Delta would still have arrived from overseas, same as it arrived from overseas in every country except one. And if anything, it would have spread faster, because they’d have gone even more fully back to normal, so there’d be a worse problem now instead of a better one.
Feels wrong to pick on such statements, but for a while I’ve been feeling the need to pick out a clean example, and this fits the bill. Also points out an important dynamic – local containment only matters for the medium to long term up until you cycle strains. There’s a strong instinct to contain the virus ‘in case it mutates’ but if it mutates elsewhere all your containment efforts mean nothing, so this only matters to the extent that you stop the mutation from happening at all, anywhere. Which is an important consideration, but not for stomping out the last few cases in one place while things continue to rage full blast in others. Much better to help out those other places.
In Other News
Scott Alexander’s post Things I Learned Writing the Lockdown Post is excellent and from my perspective is much better and more interesting than the actual lockdown post. I don’t have the bandwidth to respond properly this week, so noting here that I haven’t done so.
There’s this great highlighted comment at AstralCodexTen and I have nothing to add:
In the monthly links post at ACX, Scott also points to the poll that showed remarkable support for permanent lockdown in the UK:
But then reminds us that if you ask the questions with slightly different wording, people act more sane, and a permanent lockdown then only gets the 3% support you would expect from the Lizardman’s Constant:
They have a graph but it’s hard enough to read as it is so I’m not putting it in directly.
That makes this most of all a manufacturing consent story. Merely by changing a few words and giving people the correct word associations, you can get many people to agree to give up their freedoms and way of life, permanently. That’s scary. Not all of them, not quite this easily, but quite a lot of them.
You love to see it: UK changes guidelines to emphasize outdoors and de-emphasize surfaces.
Standard disclaimers that this like everything else is in no way medical advice and not to do anything illegal, but also this happened and further investigation seems logical:
I am not the biggest fan of psychedelics in practice under current conditions, but there’s a ton of potential upside. Our refusal to investigate their potential properly, for this and many other things, is a colossal expected value error, potentially our biggest one.
Incentives matter, so this is mostly great (via MR), but remember that if it’s $200 to get them to sing it might be considerably more to make them stop:
Incentives matter, dominatrixes requiring vaccination for dungeon entry edition. Seriously, incentives matter, stop pretending this is all so difficult.
The standard check for whether mask mandates are back says yes:
Not Covid
The lighter side presents:
Interesting whether or not they are transitive survey results of the week:
Taken together to see what happens, these imply that about 90% of people think billionaires have lives they’d rather live, and about 70% support for the superiority of the life of the True Philosopher even when you exclude the 21% who implicity endorse it by already claiming to live it. Of course, Robin is an economist and Agnes is a philosopher, and have followers accordingly, but let’s not let that ruin our fun.
Especially given this:
Mostly I find this rank ordering sensible. Olympic, Pulitzer and Academy Award winners get the glory but their overall lives don’t seem like they should automatically be all that tempting to most people, whereas billionaire or nobel prize winner seems a lot more tempting. I’d like to live in a place where greatness was widely considered worth its price, so I worry about people not seeing things that way.
The other thing to observe is that this implies that for the samples in question, life is pretty damn good. If it wasn’t, there would presumably be a much bigger willingness to switch tracks to people who very clearly ‘made it’ and have a lot going on. I tend to agree. My life is pretty great, too, whether or not I count as a true philosopher.