Amidst all the insanity you recount, there's one that doesn't ring true, the @northumbriapol tweet. The account exists on Twitter, and does appear to be the real Northumbria Police, but Twitter search does not turn up the tweet. However, I don't know how effective Twitter search is. Google search also fails to find the initial phrase of the tweet.
There is currently no outdoor daily exercise allowance anywhere in the UK, and there has not been for a long time. The full image that "drukpa_kunley" posted contains a date of 7 Jan 2021 and includes a bit.ly link (bit.ly/3qtyd24) to the "Full story", but the link is 404 (from bit.ly, not whatever the target of the link was).
If the alleged @northumbriapol tweet is genuine, the reposter has plucked old news from the past and reposted as if it was happening now. I would more bluntly describe this as a lie.
Re free speech: Social media is an existential problem to our civilization. The chinese solution of mass censorship, that the west seems to be outsourcing to private corporations' dumb algorithms, is not my preferred solution, but I honestly don't know if it's worse than the status quo.
The amount of misinformation I see forwarded even on my family whatsapp group is awful. Not even the older members of the family really buy it, but it definitely contributes to cynicism. Then there's the Q horror stories, crazy conspiracy crap and so on. This is not sustainable, society can't function with constant disruptive weaponized propaganda being thrown at us.
Maybe the Taiwan strategy of having an official government meme police that doesn't ban fake news, but sends out official responses to it very quickly can work. Maybe not. I feel like the US government, for instance, doesn't have the popular trust that the Taiwanese government has to pull something like this off.
I'm terrified by the idea of serious mass censorship, but misinformation is tearing apart western democracy. Maybe I'm being overly dramatic, maybe us younger people are more resilient. Then again, zoomer/milennial online mobs for dubious causes spring up all the time as well. I think it's wishful thinking for younger folk to say fake news is just a boomer problem.
Something needs to happen. The truth is not beating falsehood by a wide enough margin(or sometimes at all!). Dismissing this as just 1984 ministry of truth memes is silly. Anti-vaxx shit alone has probably killed tens of thousands of people. Stupid Q conspiracies led people to storm the capitol in the US. This is only going to get more severe as time goes on.
If we don't want the world to adopt China's model, we need to be very serious about creating an alternative.
Good points. I think we should compare the two worlds (China model vs. free speech wild west) more explicitly to see how they fare. My intuition right now is that I'd vastly prefer the free speech wild west to the china model, even if this gets tens of thousands of people killed on the regular because of believing stupid memes. Basically, as bad as that situation is, totalitarianism seems a lot worse... But I'm not sure.
I agree with you that social media is an existential problem to our civilization. In my mind, it is as dangerous as climate change, yet taken far less seriously.
However, I think that the west/China dichotomy is a false one -- there is likely a way to evolve the (western/democratic) system as it is into one that continues to allow the free flow of information, and at the same time limits harmful information. It seems easy to discount this because social systems take much longer to develop and implement than, say, a new car design. I hope that, given how fast the Internet evolves, we won't have to wait long for an alternative to appear though.
How many got killed after the population supported invading Iraq based on Colin Powell's very official little lies that Iraq had WMD and was linked to 9/11? According to Wikipedia:
U.S. military deaths: 4,576
Iraq excess deaths: aournd 500,000 according to Lancet and PLOS Medicine, including at least 100,000 violent deaths
I believe the anti-intimacy Olympic beds are not a thing - or at least, I've been convinced that it's just a strange bed design and not an anti-covid measure in itself: https://twitter.com/McClenaghanRhys/status/1416567768938291203
You don't really address the dosing controversy on vaccine efficacy, except mentioning that you think it's dumb to worry about, but there is something potentially concerning there. There's some evidence that the dosing interval is causing some differences between the vaccine efficacies reported in Israel and the UK. This discussion full of immunology science words I don't understand says there is a measurable difference in response to delta for short vs long doses.
The results from Israel, which used a 3-week dose interval, look bad, and contrast with the UKs results, which were (mostly) on 8-12 week intervals. But there are apparently sampling biases which mean the Israel data might not be fully reliable. See also here.
Overall, I'm not sure what to make of this - even if 3-week intervals is generating strong levels of neutralizing antibodies and won't become highly infectious or severely ill, it seems important to know if 2 Pfizer gives ~65% or ~90% protection. Unfortunately, I don't think we'll see studies on this for a while, so if anyone has better interpretations of this data it would be useful.
Is it a good idea for two-dose vaccinated people to get a third dose? I know there won't be an "official" Very Serious Person answer to this question for a while, but I'm interested in knowing the best course of action to take as an individual now, given the info we have.
The most relevant data I've seen on third dosing is from Pfizer: https://cdn.pfizer.com/pfizercom/2021-07/Delta_Variant_Study_Press_Statement_Final_7.8.21.pdf?IPpR1xZjlwvaUMQ9sRn2FkePcBiRPGqw
"Pfizer and BioNTech have seen encouraging data in the ongoing booster trial of a third dose of the current BNT162b2 vaccine. Initial data from the study demonstrate that a booster dose given 6 months after the second dose has a consistent tolerability profile while eliciting high neutralization titers against the wild type and the Beta variant, which are 5 to 10 times higher than after two primary doses."
Given the above, I'd probably try to get a third dose right away, except that I'm unsure about:
Would greatly appreciate anyone's input on the above!
See also this question, which asks the same question and comes with a $1000 bounty for the best answers: https://www.lesswrong.com/posts/fBGzge5i4hfbaQZWy/usd1000-bounty-how-effective-are-marginal-vaccine-doses
Strong +1 for writing the post-mortem -- there are incentives not to write that kind of thing, but I appreciated it. I also get value out of your weekly posts, so thanks for writing those.
That being said, I do have a few minor quibbles with the post-mortem. I think I interpreted your December (and future month) claims more strongly than it sounds like you interpreted them.
I haven't re-read all your posts carefully to check for places you might have said this, but I don't remember seeing you say in the 1-2 months after your "We're F***ed" post that you thought it was significantly less likely that we're f***ed. E.g. I commented on a January post https://www.lesswrong.com/posts/Rhy5g75NdRKdw9ibB/?commentId=2TjkS4XLA5PaAjoxG#2TjkS4XLA5PaAjoxG saying that the UK evidence seemed pretty strong that we were possibly not f***ed.
I was also somewhat surprised that in the post-mortem, you said you thought the 70% prediction evaluated to false.
From that post:
The new strain has rapidly taken over the region, and all signs point to it being about 65% more infectious than the old one, albeit with large uncertainty and error bars around that.
I give it a 70% chance that these reports are largely correct.
There is no plausible way that a Western country can sustain restrictions that can overcome that via anything other than widespread immunity.
I haven't looked into the details of this much at all since February, so I don't have strong takes on whether the UK strain is closer to 40% or 55% more infectious (and "more infectious" can be defined in different ways). Comments on this metaculus question https://pandemic.metaculus.com/questions/6089/50-transmissible-variant-to-infect-10m/ suggested that people, at the time at least, believed the number was likely close to 55% (note: the overall probability on the linked question also includes the probability of other strains infecting >10M people by June 2). There's also a decent amount of room for different interpretations in "largely correct," and a 10% difference in infectiousness matters a lot, but at the time at least, I would have predicted that 55% was close enough to 65% to hit your "largely correct" bar.
One reason I pushed back on some of your posts in Dec - Jan is that I thought the post was directionally wrong for the LessWrong community (I think LessWrong readers as a whole were much too cautious as of Dec 2020). I think people in the community deferred to the reasoning of "We're F***ed" some, and that it would've been better if you had more quickly updated / told people that you had updated.
Overall though, I appreciate you writing these posts, so I hope my comment doesn't come off as too critical, and thank you again for doing that.
I agree that 55% would be an ambiguous evaluation, but 40% is substantially different than 65% and I've been using 40% in my recent models. Central mistake is the same in both cases.
I don't remember what my update timeline was, I'd have to go back and look. Makes sense I would be too slow.
Anyone interested in elaborating about Ivermectin? I've been hearing drama over the medication for quite some time but am unaware of the details.
I've made several changes, please reimport when you get a chance. Nothing urgent or that would change the central point.
I keep seeing references to 'long covid' by smart people, usually in the context of "we need to confirm what the effects are" but have never seen any real evidence from obscure or mainstream sources that it's something worth thinking about much. Surely if it were a real and important thing it would be identified and proven as such by now?
At this moment it strikes me as something that's probably either bullshit or a minor consideration until further evidence emerges to the contrary, but smart people continue to mention it. What am I missing?
BBC: https://www.bbc.co.uk/news/health-57584295
The Times: https://www.thetimes.co.uk/article/why-is-britain-now-the-capital-of-long-covid-grjpvzfvw
There's a good chance that the numbers are overstated because of methodological difficulties, but it's not obvious, and the numbers are high enough that it would be worth concern even if they're 50% overstated.
Also, reddit is full with scary stories about Long Covid. Obviously that doesn't mean much because you get scary stories in any data set with tens of millions of people, but I think it's quite telling that a lot of people who self-declare as having Long Covid report having messed up senses of smell (e.g., strawberries tasting like burnt tyres). That's not usually a sign of normal depression or burnout. It's clearly Covid related, and it seems to happen frequently enough to produce reddit communities filled with such posts every day, and the media did report on it, and the symptoms seem to be connected (e.g., the people who report the long-lasting loss of sense/taste also have other fatigue-related symptoms, which seem to have gone up in people with past Covid as well).
Good points.
Notably, those studies are still based on surveys and self-reports.
Compare supposed long lyme disease or previously, supposed candida infection. In those cases a lot of people self-report various general, common symptoms like tiredness. In neither case is the disease medically recognized. Rather, its existence is doubted by medical authorities. In addition to these two, I there's a series of past similar scares, with the same properties. These scares include at least electricity oversensitivity and worries about mercury dental implants.
In all these cases it seems likely that there is no physiological long-lasting disease. Rather, because belief in a long disease spreads, people start to wrongly attribute their general symptoms and issues in life to it. Things such as tiredness, depression and pain get self-reported in large numbers.
Now, it seems to me somewhat likely that long covid will turn out to be in the same category. There is a lot more self-reported cases of long covid than long lyme disease. But belief in long covid is also a lot more widespread.
Why do medical authorities not apply to same skepticism to long covid as they did to eg long lyme disease? One possibility is that there's a perceived (maybe justified) need to spread beliefs about how covid is dangerous, and so a different standard of evidence is applied.
Your theory doesn't explain the prevalence of highly unusual Covid-specific symptoms among the mix that makes up Long Covid (I'm thinking of strawberries smelling like burnt tyres)
The persistence of anosmia doesn't entail that other symptoms are caused by Covid. (IIRC the relevant cells in the nose take a while to regenerate). Though I agree this provides some evidence that Covid is the cause.
There's a second plausible mechanism with Covid: It affects blood vessels and lots of organ systems at once, so lasting damage causing fatigue seems to make sense
This predicts that you'd find organ damage in these patients. Are there studies showing clear organ damage in people with mild cases 6 months later?
Some people's Long Covid symptoms are too outlierish in their severity to be anything that develops normally. E.g., people who used to be highly into sports report that they get out of breath just climbing stairs, and that this persists for a period of years. My impression is that this sort of thing never just happens without an identifiable cause.
I disagree. This does happen without an identifiable cause.
The persistence of anosmia doesn’t entail that other symptoms are caused by Covid
But it raises the probability.
I was curious and thinking about testing.
If I was still the kind of jerk I was in my 20s, maybe I’d find some spreadsheets shared with me and add “Pfizer vaccine causes impotence” or whatever.
(Would save a copy prior, of course)
It'd be more fun to mess around to find out what triggers it. If "Pfizer vaccine" was enough, you could get people mad about losing documents for pro-vaccine comments.
With regard to Eliezer's point about early-dated vaccination certificates...
The conformity part can go from "this certificate means person is high-conformity" in liberal areas to "this certificate means person is low-conformity" in conservative areas.
Delta progresses more quickly, and all else equal, that should make you less worried about R than you previously were. But I find it plausibly that it's doing both: it's scarily infectious and it progresses more quickly. Depending on the methodology of estimating R, it doesn't necessarily lead to overestimates if one variant progresses more quickly. Your methodology could be to simply trace infections and count how many times a virus was passed on from the earlier generation's host.
There's some evidence of scarily high infectiousness. From Australia, we see that it apparently happened twice that there's CCTV footage of people walking past each other (without mask) and infection happening within 15 seconds of passing. This wouldn't be too surprising if that's all the footage we had about scarily quick infections from major outbreaks in the US or the UK – large numbers imply bigger coincidences. However, the Australia outbreak is young and scarily quick infections happening twice implies that they must be rather common.
One thing I'm confused about is the UK's recent case numbers: They seem to have slowed down a lot. It's too early to tell and I think there's a good chance the growth picks up again, and it'll look very different next week. But there's a chance that the UK is close to the ceiling already, which would be good news, and probably some evidence that experts overestimated the R of Delta variant, because many experts were predicting >100k or even 200k daily cases over the summer, and this may not happen if the apparent slowdown is real.
(Alternatively, maybe society is really segmented by now and many people are intent on not catching the virus, so saturation is only reached within populations that are comfortable with quite a lot of risk. This could still lead to a slowdown, but not for ideal reasons.)
The 15 seconds transmission (if it's reasonably common and doesn't involve one person coughing or sneezing in someone's face) suggests a quite different infectiouness profile than other variants. You'd expect massive superspreader events from public transport, bars, and events. You'd expect very few people to be infected by family members (because they are exposed to so many people for 15 seconds). I'm not ruling this out but it sounds a bit unlikely based on reports of Delta spread so far.
I've seen a bunch of reports that feel intuitively consistent with this. E.g., superspreading around the Euro finals ("the Wembley variant") and accounts from weddings that I vaguely thought were outdoors, but that could be a false memory. I'd imagine that people would continue to get infected by family members (at least ones that live together) because the secondary attack rate would be really high with such an infectiousness profile. And I've also seen some claims from Israel or Australia about near-100% secondary attack rates, but they seemed really anecdotal, so I don't know. (I expect that it's already possible to gain a lot confidence about all of this by doing a systematic screening of sources/reports.)
That the same 50% of the unwilling believe both that vaccines have been shown to cause autism and that the US government is using them to microchip the population is suggestive that such people are not processing such statements as containing words that possess meanings.
Yes, but you're missing the obvious. Respondents don't have a predictive model that literally says Bill Gates wants to inject them with a tracking microchip. They do, however, have a rational expectation that he or his company will hurt them in some technical way, which they find wholly opaque.
Likewise: do you think that the mistake you mention stemmed from your impatience, which makes you seem blasé about the lives of immunocompromised people like myself? Because, those lawmakers you chose to bully were all vaccinated, so they were engaging in the exact same behavior you just criticized LA for trying to ban. You also just implied, earlier in the post, that if people were less impatient, we'd be largely done.
I don't see how we're saying different things here - we both agree that the respondents aren't evaluating the statements as containing words having meanings, they just have negative affects and that's that.
I also don't see any charitable way for what I said about the plane ride to count as 'bullying.' Also, equating wearing masks on a jet (when there's still a national mandate for mass transit, and also there's clearly a lot of people in a tiny space for a long time) to a universal mandate for masks in indoor spaces is weird.
Because, those lawmakers you chose to bully were all vaccinated, so they were engaging in the exact same behavior you just criticized LA for trying to ban.
I don’t think Zvi was bullying them, more so just trying to highlight the hypocrisy of imposing mask restrictions on a population and then ignoring them yourself. It’s true that these particular lawmakers were not the same as the LA leadership, but the Democratic party as a whole is absolutely guilty of preaching/mandating one behavior publicly, and then privately flouting it themselves.
The real issue is that this kind of behavior makes the whole enterprise appear understandably suspect. Which is it: are masks necessary, in which case why are you taking a risk with your own life? Or are they unnecessary, in which case why are you supporting mandates? The conspiracy theorists‘ dream, really.
I am deeply confused how a serial interval can be negative. If I understand the words involved that means you spread it on to someone who gets their symptoms before you do?
If I understand that correctly, it means you're breathing out infectious levels of virus days before you cough / notice that you are sick.
(I'm confused about your confusion, because I thought the negative serial interval of COVID was one of its most striking features, and the reason why many of the old 'control system' things failed; like, people were used to "if you feel fine you are fine" and wouldn't accept "everyone needs to act as though they could be sick, because you won't know whether or not you're infectious until after the fact.")
Yes, I get the idea that you can spread the disease before you show symptoms, but this would be the person you infect showing symptoms before you do, as an expectation, which does seem super weird.
Or another framing: The question is, how long is the time between being infected and then infecting someone else? And the answer might be smaller than the time before you show symptoms, but if it's negative the virus is doing something involving time travel.
The 'generation time' is the one that can't be negative. Suppose Alice gets infected on day 1, infects Bob on day 2, Bob shows symptoms on day 3, and Alice shows symptoms on day 4. We end up with:
Or another framing: The question is, how long is the time between being infected and then infecting someone else? And the answer might be smaller than the time before you show symptoms, but if it’s negative the virus is doing something involving time travel.
They seem to be referring to the serial interval between symptom onset. Which indeed can't be negative on average. But they write it was only negative in 21.6% of cases. And there is no rule stating there can't be cases where it's negative (as long as you have transmission before symptoms).
If you see a plane crash reported and don’t know that crashes always get reported, it’s good news because you learn crashes are rare enough to be news.
[...]
Then again, there was also this, in the comments last week:
For the record, the wedding I went to did end up in the news.
The Dutch festival actually was a 2-day event with a total capacity of 10,000 people per day. But it is reasonable to assume that some amount of people attend the first and then the second day, so the total number of participants is lower than 20,000 and correspondingly the rate of infection is unknown but somewhere between 5% and 10%.
I'm not sure why you think it's not legal for employers to ask about vaccination status? I can't think of a law that would prohibit it, and the EEOC says it is legal: https://www.eeoc.gov/wysk/what-you-should-know-about-covid-19-and-ada-rehabilitation-act-and-other-eeo-laws#K
Vaccination status is one thing, asking in 2025 whether you were vaccinated in August 2021 is another.
There is a tricky free speech issue around deliberately lying. At the moment, you can construct a major lie and publish as widely as you like without consequence provided it is not defamation. Note that I am not talking about propogating someone elses lie that you believe to be true. If I look at Fact checkers, I see some monstrous stuff that is plainly a deliberate creation. Someone's belief that vaccines are bad, means they feel at liberty to make up crap to support their viewpoint (for instance). I'd like to see a consequence very much like defamation laws that could be applied to malicious lies that demonstably inflict harm (with the same kind of levels of proof that apply to defamation). Deliberate lies are risk to intelligent public discourse.
The essence of free speech is the ability to criticize government members and policy without fear of reprisal. It does not give the right to defame government members (at least here in NZ). Nor should making up lies about government policy be allowed as free speech.
Who do you want to be in charge of deciding which lies were 'plainly a deliberate creation' and have 'caused harm', vs which lies were 'probably genuinely believed as opposed to deliberate lies' or 'did not cause harm because, while lies, they misled people in good directions rather than harmful ones'?
As Phil says, we already have defamation laws that draw similar distinctions. For instance, in many jurisdictions a statement can't be defamatory if the person making it made it in good faith and reasonably believed it to be true.
In those cases it's a kinda-randomly-chosen jury, guided by a court proceeding with lawyers on both sides and a judge in charge, that has to make the call. We as a society seem to have decided that that gives fair enough results. Maybe it would work much less well for an offence of spreading malicious lies (because maybe it would be more tempting for governments to put pressure on the courts, or maybe it would more often happen that the jurors' political prejudices got in the way of making a reasonable decision) but it's at least plausible that it would be net beneficial anyway.
I think it is civil proceedings just like defamation. The defense against "making stuff" up obviously is your source.
Has anyone found a good explanation as to why cases decline so rapidly in places where the Delta variant took over?
{kind=link}
Delta has taken over, and cases are rising rapidly, with a 58% rise this week after a 65% rise last week. There’s no reason to expect this to turn around in the near term.
Three weeks ago, in One Last Scare, I ran the numbers and concluded that most places in America would ‘make it’ without a big scary surge from Delta. It’s time to look at what went wrong with that calculation, which I believe to be a failure to sufficiently integrate different parts of my model.
Then there’s the question of what we are going to do about this, and whether we are going to destroy some combination of free speech and the ordinary day to day activities that constitute our lives and civilization, perhaps indefinitely, in the face of this situation. Such collateral damage has the potential to be far scarier and more deadly than the direct threat from Covid-19.
Let’s run the numbers.
The Numbers
Predictions
Prediction from last week: Positivity rate of 4.7% (down 0.1%) and deaths unchanged.
Result: Positivity rate of 4.4% (down 0.4%) and deaths decline by 5%.
Other Result: Positive test counts rose by 58%, versus 65% last week.
I do not understand the divergence between positive test rates and case counts that we see here. This implies that the number of tests is scaling with the number of cases, but that wasn’t true earlier, and also there’s a lot of testing that takes place out of an abundance of caution or to provide the necessary evidence and/or paperwork in various contexts, where the tests clearly wouldn’t scale. So this is weird.
In any case, it seems pointless in this context to make a positivity rate prediction instead of a case count prediction, since it doesn’t tell us what we want to know. Thus, I’m switching to predicting case counts.
There’s no reason to think cases won’t continue to rise in the near term. Control systems should be kicking in and Delta has mostly completed taking over, so the rate of increase should continue to slowly decrease. I’m going to predict a 50% increase, down from 58% this week and 65% last week.
Prediction for next week: 360,000 cases (+50%) and 1845 deaths (+10%).
Predictions will be evaluated against data from Wikipedia, after correcting for obvious data anomalies.
Deaths
There’s no sign yet that people are dying from the new wave of cases. Most of the rise in cases came in the last two weeks, so we wouldn’t expect a dramatic increase yet, but seeing a 5% rise over the last two weeks is still at least somewhat reassuring that what we’ve seen in places like the UK, where the IFR was dramatically reduced versus previous waves, will also happen here.
If we don’t see a big rise in deaths within the next two weeks, that will be both very surprising and quite excellent news, as there will have been enough time for at least some of the new cases to have resulted in deaths. By three weeks from now we can be confident what new normal we are dealing with, at least as long as the hospitals have sufficient capacity.
The cases remain the story.
Cases
Last week was a 65% increase, and this week was a 58% increase. Delta has now mostly taken over, so differences are some combination of reporting, timing and testing details, seasonality changes, and control system adjustments. We should expect some people to alter their behaviors by now, and that will accelerate as cases pick up.
Either way, we have a 60% increase week over week as the new baseline, which would represent R ~ 1.4 based on the old assumption of a five day cycle. That remains consistent with the 2.2 multiplier on Delta versus a 1.4 multiplier on Alpha, plus the control system having adjusted to be stable under Alpha.
Vaccinations
Vaccination rates are now roughly stable at about 500k/day, so about 1.5mm people/week going from unvaccinated to vaccinated, or about 0.4% of the population, and a resulting 1% or so decrease in R. If we think Delta is still on a five-day cycle, that’s 1.5% less case growth each week. If Delta is on a three day cycle, it’s 2.3% less case growth each week. More on that in the Delta section.
The good news is that we are seeing more Republicans stepping up and telling their constituents to get vaccinated. That, combined with the threat from Delta, should help, despite the efforts of the Ministry of Truth. More discussion in that section.
Not Necessarily the News
When X is reported on the news, we learn at least three claims to evaluate:
Depending on your prior knowledge and model, the same news report can change your world model in opposite directions, and often people get this calculation wrong.
If you see a plane crash reported and you know the media reports most plane crashes, that’s bad news, but it’s not importantly bad news, and it at least means there wasn’t worse news crowding it out. If you see a plane crash reported and don’t know that crashes always get reported, it’s good news because you learn crashes are rare enough to be news.
This brings us to this week’s reports of infections taking place at a wedding.
This led to a bunch of reactions that were at core like this one:
Which in turn is doubtless causing a lot of this:
One could also observe that one person dying, or six being infected, was news, and worry perhaps even less than before, given how many weddings there are.
Then again, there was also this, in the comments last week:
Twice is at least suspicious, and these two do seem to be close together in a meaningful way. So it’s at least a little bit news.
Similarly, we have the headline that 27 vaccinated people (it says “nearly 30” but actually it’s 27) in Louisiana died of Covid. The vaccines are so effective that 27 deaths was news, which is rather good news. If you run the numbers on Louisiana, I find roughly 900 deaths in the ‘vaccine era’ starting some time in March, so we’re talking roughly 3% of all deaths, from a group that includes most of the old people for most of that time. Yet I saw people freaking out about this, or wondering whether or not or how much they should be freaking.
We also got more data on the Dutch music festival, where it seems 5% came back infected. It seems the festival was ‘not entirely open air’:
It also involved most everyone being unmasked in surrounding bars and restaurants. So the result here is not surprising, nor is it a warning about the dangers of outdoor events, or of anything but the usual rule of ‘don’t do stupid stuff.’
Delta Variant
I always wonder in cases like this, how did they think a number like 83% gets distributed, and do they think a very slightly unequal distribution is somehow scarier or worse? Similarly, was going from 50% to 83% in two weeks unexpected somehow?
If you assume we started with a 50/50 split with Alpha versus Delta, and then there are three serial intervals since July 3, you get 79%. So this is very close to what you would expect based on my baseline estimates (with no loss of effectiveness from the vaccines, or very little), which is interesting in light of the discussions on Delta potentially being faster, which I’ll talk about next.
BNO Newsroom offers this graph for easy reference, which has >50% in the July 3 bucket and thus has growth almost exactly in line with expectations. And the previous two week period was a slower takeover than one would have expected from the same model:
Also, OurWorldInData turns out to graph this the same way it graphs everything else, and I find their presentation very clean and easy to read:
An interesting and hopeful theory that came up was that Delta might be spreading so quickly in large part because it is faster. Under this hypothesis, rather than there being an average of five days between the time you catch Covid to when you give it to someone else, that interval could be as small as two days. That makes physical sense if the viral loads are much higher, as Delta would need less time to multiply in a new host before being able to spread.
If this was the case, then what looks like much higher rates of infection in graphs, and in the type of analysis that was run last week, is a lot less scary, and the actual R will be much closer to 1 (in theory, in both directions) than I calculated. Doubling every five days previously would have meant R ~ 2, but if that’s two and a half cycles, then it means a much more fixable R ~ 1.31. What otherwise would look like a ‘we’re f***ed it’s over’ scenario might not be one.
What’s the evidence for this? We have this study out of China:
I am deeply confused how a serial interval can be negative. If I understand the words involved that means you spread it on to someone who gets their symptoms before you do? In which case, wow, that’s quite the rapid spread.
It goes on to say this about R:
If R0 went from 2.2 to 3.2 in this type of setting, that’s less than a 50% increase from the original, so it’s only ‘in line’ with the 97% increase reported by Finlay in the sense that they both observed the same rate of increase in cases, except Finlay assumed the old timing of infections and this new study believes things have sped up a lot. Thus, what would have been 97% is now slightly under 50%.
Their graphs are quite good. I wish more papers were 2 pages long with this much useful information:
I’m not fully sold, but it seems likely this is right. We are seeing super duper fast spread of Delta in some places, and not in others, and in some times and not others, such as when India went suddenly from an out of control epidemic to everything stabilizing quickly. Speeding up transmission makes all of that make a lot more sense.
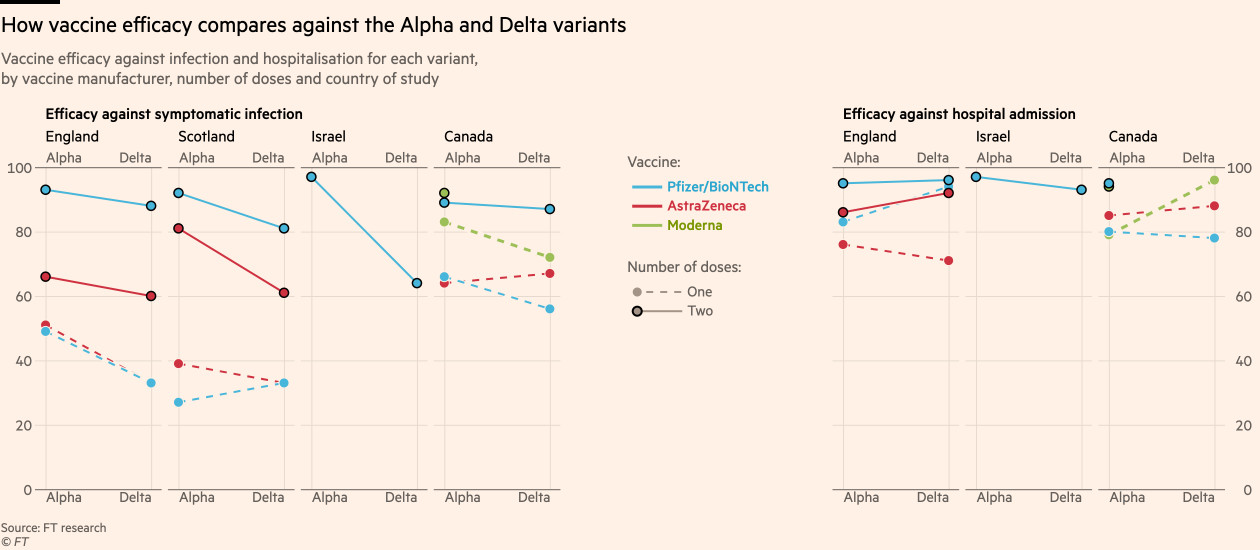
A comment last week pointed to this study of vaccine effectiveness against Delta. I believe it had already been incorporated into the claims assessed last week, but good to explicitly note the primary source. I’m reproducing the bottom-line sections in full, skip if you don’t want to dive into the details.
In general, it’s potentially highly misleading to compare the vaccinated to the unvaccinated in the wild, because the two groups differ in a lot of ways. I’m not entirely sure which direction this goes, as the vaccinated start out with safer behaviors but then change behaviors based on being vaccinated.
Here, we can compare measured vaccine effectiveness between different strains. The obvious worry then is that there could be a difference in which populations are dealing with which strains during this period, which could skew the results as well. These are not controlled experiments. One thing that makes me more confident here is that we see other adjustments and measurements that don’t seem out of whack.
The headline conclusion is then that mRNA vaccines retain 88% effectiveness against positive tests. If we accepted this figure, we’d then need to translate that into a measure of how often such people transmit. With milder cases and lower viral loads, the presumption is that they don’t transmit as effectively, but the flip side is that milder cases mean we might be missing a larger percentage of cases, so the 88% number might be high for that reason. It also might be low or high for several other reasons.
Here’s CellBioGuy in the comments at LessWrong:
Most of the variance remains in the difference between measurements in different places, but I think all of it points to roughly the same place anyway.
The numbers will come in somewhere in the range where fully vaccinated groups won’t have outbreaks unless they partake in a lot of what I call ‘stupid stuff,’ which is basically (some combination of most of) packing lots of people tightly into indoor spaces without proper ventilation for extended periods. However, it also would mean we’re close enough to the edge that if everything went fully back to normal, we’d need more people vaccinated than we can realistically hope for in the next few months or perhaps ever.
How worried should a vaccinated person be about Delta?
In terms of death, seriously not very much, vaccinated people don’t die of Covid and Delta doesn’t change that. Thread points to a few different claims about whether Delta is deadlier and by how much, but it’s definitely not enough to overcome the vaccinations or even put much of a dent in them.
The question is entirely one of the unknown unknown risks of Long Covid. Getting data on this, or being confident in a position, is incredibly hard, whether it’s on how big the Long Covid risk was to begin with, or how much the vaccines reduce that risk. It would be completely biologically bizarre if the risk wasn’t greatly reduced by the vaccine the same as everything else, but it’s still enough of a worry that one would strongly prefer not getting Covid, if that was an option.
I wish I could do better than that, but I really can’t give one, given what I know. My guess is that we’re talking about a small but non-zero chance (3%?) of some amount of lasting effects of some kind for the vaccinated, most of which are minor and temporary, but yeah, who the hell knows.
For young kids, that’s even more true – the danger is purely Long Covid. There’s a good ‘what’s up with Delta and kids’ analysis up this week, although it doesn’t offer us anything concrete that’s new, and it points out that the Long Covid risks haven’t changed and that other diseases also have similar long tails, we just don’t talk much about them. And that even with unmasked schools and lots of vaccinations elsewhere, we’re not seeing an explosion in cases among those schoolchildren too young for the vaccine, as a percentage of the cases in the population when there’s a Delta wave in the UK:
It is well known that city living leads to more infectious diseases than non-city living, to a very large degree. There’s a small long tail for many of those diseases, where people develop long term problems. One of the periodic reminders, as we move into the next phase of the pandemic and beyond, is that if you are worried about Long Covid as a vaccinated person, why aren’t you completely panicked about living in a city?
That brings us back to the calculations. The spread of Delta in the United States as a share of cases is exactly in line with the 2.2 vs. 1.4 difference from Alpha to Delta, as of earlier this week, which does not leave room for vaccines to additionally lose effectiveness. Then, if it turns out Delta replicates faster, that changes the math once again.
One Last Scare: Re-Evaluation
This week, I was persuaded to add a post-mortem to my big We’re F***ed, It’s Over post from the end of 2020. Reading it over again, I believe the core logic of that post was solid – we were not capable of adjusting the control system sufficiently to contain a 65% more infectious strain in time given the expected rate of vaccinations. I predicted a 70% chance that we had such an infectious strain and that if we did, we would face this crisis and have no reasonable options.
It didn’t happen. Instead we had a 40% more infectious strain, and faster vaccinations, which combined as that post’s model said it would, to prevent the wave. We did better than I would have expected even then, with cases coming down much faster, so there was even more going on than that. In any case, the prediction was too confident, and didn’t properly adjust for uncertainty over speed of vaccinations or seasonality. Perhaps there was even some degree of self-preventing prophecy when you combine it with others’ similar warnings. I do think giving the scenario less than a 30%-40% chance would have been more wrong than giving it a 70% chance, but that numbers over 50% were too high.
This time around, I predicted:
It does look like masks will be around for a while, and might be making a comeback – Biden is considering reinstating them in many situations, or at least trying to do so, and many schools look poised to torture their students this way, and several jurisdictions (including Los Angeles and Las Vegas) are bringing back indoor mask mandates already on their own.
We also aren’t seeing that many calls for anything beyond mask mandates yet, but I do see the beginnings of ‘schools can’t be open’ talk as well. I would like to think we’d never let that fly at this point, but perhaps we would, at least in some places. I do think that if you’re a parent in such a place, and they do try to put your kid in ‘remote learning,’ you should find an alternative even at an extreme cost, and if necessary consider moving.
Regardless of all that, I know that at the time I did not expect this amount of increase in case counts, and thus my model of the future was importantly wrong. What were the errors? What has changed?
First it’s important to know what hasn’t changed: I still have Alpha at 40% more infectious (1.4x) than baseline, and Delta as 120% more infectious than baseline (2.2x). Those estimates are doubtless not exact, but I haven’t seen any reason to adjust them. So that wasn’t the problem.
Nor was the issue (as far as I can tell) that vaccines have lost effectiveness. It does seem like vaccines are slightly less effective against Delta, but I continue to believe this effect is not a big impact. Vaccinated people remain very hard to infect and, when infected anyway, poor carriers with which to infect others. This shouldn’t have moved the needle enough to get noticed.
This is reflected in the growth of Delta as a share of cases, which matches very closely what these numbers imply, and doesn’t leave room for them to be that off in either direction. Similarly, it looks like Delta plausibly replicates faster than we thought, but that probably also would mean it isn’t as infectious and has a lower R, or else the numbers don’t work out.
Thus, I do not think the prediction error was about a misevaluation of Delta. I think the error was about a misevaluation of where things stood before Delta, and what people were up to.
It’s that first sentence, where I start off R at 0.84, instead of factoring in the changes coming from the control system. With the decrease in masks worn and f***s given over the last month or so, combined with seasonality changes, the R without Delta likely went from 0.84 back to at least 1. That’s a 19% difference each cycle, or a 28% per week.
In the world where we had retained the behaviors that were cutting cases in half every three weeks, the current rates of increase would be more than cut in half, and it would be easy to see that additional vaccinations (and some amount of Delta burning out in the younger populations where it’s spreading the most) would reverse the problem before it got into crisis mode, even if our current case starts with R=1 exactly.
However, we’re not in that world, and we’re starting from a higher baseline. That mistake compounds each week, and now only a few weeks later we are where we are, with exponential growth looming quickly.
In short, I think this was mostly a pretty dumb mistake that should have been easy to spot – I knew in one place that we were adjusting things, and then didn’t make that adjustment when I did this other calculation. My models were insufficiently integrated.
The prediction here is then saying something about what happens if we return to the behavior patterns we had when cases were declining rapidly. The extra vaccinations would be sufficient, in most places, to compensate for Delta. The problem is that we’re not doing anything close to that, haven’t for some time, and it would be a hell of a thing to try to return us to that state. Even if we could, that doesn’t mean we should.
That’s also a pretty easy call to make, when one puts it that way. Delta is likely a little over twice as infectious as the original. Over half the country’s adults are vaccinated. Of course that’s enough to compensate. Easy math is easy.
Or, to do the rough calculation another way, Delta cancels out the vaccination of the first 55%-60% or so of the adult population, or the first 46%-50% of the overall population, if there’s no other source of immunity running around. We are currently at 49% fully vaccinated and 57% partly vaccinated, or effectively about 53%. So we’re still ahead, but we’re not that far ahead, and we definitely can’t go back to anything like normal unless we’re willing to accept the consequences.
From here on in, mostly the unvaccinated will be infected, and most of them will be young. Last week, we had 240k positive tests and vaccinated about 1.5mm people. With rapid weekly case growth, it won’t be too long before we’re giving immunity to our unvaccinated youth the hard way, via infections, faster than we can vaccinate people. It’s not the preferred solution, but it does work, and it works fast, especially since it tends to kick in about when other control systems also kick in. Which is why we see rapid increases time and again suddenly turn into rapid declines all of a sudden.
The question is, to what extent are we willing to accept those consequences, versus willing to accept the costs of not accepting them? There’s no longer a reasonable expectation that if we kick the can far enough down the road that something will change, and the consequences of permanently kicking the can seem far, far worse than the consequences when the can is not kicked.
Speaking of which…
Ministry of Truth
So, this happened:
Google is blocking your access to documents, based on them containing the wrong statements about vaccines. While this turns out to (for now) likely not involve private documents, and only stop the sharing of information, you should presume both that your documents in Google Drive are not private when it counts, and also that you could lose access to them at any time, especially if they they are technically ‘shared’ as many of mine are. It’s not as scary as I originally thought, but it’s still scary.
I already knew about such issues, but this drove it home. More new is this (link to video):
There’s also this:
Mike’s full-post take on the situation is here.
A call from the executive branch, for social media platforms to coordinate, and if you’re banned on one of them for ‘misinformation’ you need to be banned on all of them, or the government will take action to break up this private monopoly of a public platform. Also, they need to ‘work harder’ to ‘fight the spread of misinformation’ via censorship and bannings of this type, or again, they will take action to break up this private monopoly of a ‘public platform.’ If they don’t do that, they are ‘killing people.’
He tried to walk it back:
However, that’s not how the language works. It is how the language of power works, where one makes one’s statements as ambiguous as possible and states one’s message implicitly whenever one can, so that one can get the message out and then deny sending it.
Meanwhile, from NPR via that column, the following definition of ‘misinformation’ when a Bad Person is providing the information:
Misinformation, it seems, could mean anything that gives an impression the Powers That Be dislike.
Such policies have often taken aim at anything that ‘contradicts the CDC guidelines’ or used other such principles, despite such guidelines often being obvious nonsense.
So, that happened. As usual, think about this apparatus, and this move, in the hands of the outgroup rather than the ingroup, or the hands of the fargroup, if you think that it might possibly ever not be one of the worst possible ideas.
As gentle reminders from earlier in this epidemic, this ‘misinformation’ would at one point have included the fact that masks work, or that the virus could have come from a lab, or that we could expect to perhaps have a vaccine by the end of 2020, or if you go back to February that there was even a Covid-19 problem to begin with or that one should prepare for it, because that’s not only false, it’s also racist. Or that Covid-19 is airborne, or that surface cleaning wasn’t all that important. And that’s purely from the current pandemic and without thinking about what the outgroup would have done with those levers if it had the chance.
Under such a regime – or under the current regime that existed at the time, even – if my posts had been placed on social media, I’d have been banned from all of them many times over. That’s where things already are, now. What happens when ‘misinformation’ increasingly becomes whatever the executive or the media narrative decide they don’t like? And then the executive decides he doesn’t like those who don’t like them, or are saying politically inconvenient things?
Many have noted that the call for government-directed censorship of social media is not only far along on the road to authoritarianism and the end of freedom of speech, it also doesn’t have much prospect of a big impact on its supposed target either. Link is to one such thread. It’s almost as if the government and ingroup establishment are using the ‘emergency’ and the excuse of the pandemic in order to further their goal of becoming the thought police and telling us what we can and can’t say to each other.
Things offline are not entirely better, but in the interests of illustration by example and a desire not to cause a distraction, I’ve censored the example I had previously put in this spot from the past week. Stay on target.
Vaccine Hesitancy
What’s actually going on with vaccine hesitancy (link to CNN post)?
When we ask whether persuasion works, I mean, of course it works. The issue is that you’re not the only one doing persuasion, and also you’re not doing that great a job of it, in the sense that this thing has been massively botched several times over. Persuasion matters, doing it better matters, and what we got reflects how we did at it. And yes, every little bit helps and we might be close to a tipping point.
You know how uninterested we are in persuading people? Not only did we suspend the J&J vaccine over nothing, and recently put another warning on it over another nothing, we’re not even bothering to fully approve the vaccines, with all that this entails. Let alone the other low hanging fruit mentioned at the link.
Kelsey puts this well:
Or even more bluntly:
Let’s not pretend we’re taking this seriously. Matthew also notes this:
This is no different than anything else. Vaccine persuasion is about persuading others that we are Very Serious People who have made the proper sacrifices, rather than asking what would work.
A better question is, how much does persuasion at the margin, now matter? The persuasion that mattered most largely happened by January. Those who were persuaded by then mostly stayed persuaded and got their shots. Those who weren’t largely didn’t change their minds later. But why would they? Yes, some new evidence was presented that vaccines were safe and effective, but also the problem seems far less urgent now. Until that changes, it’s not like we did some great persuading and it didn’t work.
One big piece of evidence is that most old people went ahead and got vaccinated.
This looks like a world in which people are doing a calculation to decide whether to get vaccinated – they’re simply doing a different calculation, where the decision is less obvious, and those who most need the vaccine mostly still end up getting it.
This in turn implies that much of the remaining ‘hesitancy’ or even refusal isn’t ‘I’m never doing this no matter what’ and it’s more like ‘I don’t have enough skin in the game so I’d prefer to play it what looks to me like safe and/or not bother and/or not deal with the temporary side effects and/or continue signaling to my in-group.’
Which is great news, because if Delta ends up everywhere, where chances of getting infected if you’re not vaccinated get very high, then one would expect a lot of people to cave and get vaccinated rather than accept getting infected.
And that’s despite some pretty out there world models, even if you subtract Lizardman’s Constant:
That the same 50% of the unwilling believe both that vaccines have been shown to cause autism and that the US government is using them to microchip the population is suggestive that such people are not processing such statements as containing words that possess meanings. They’re simply taking the opportunity to say ‘rar, vaccine bad!’ in any way that’s presented to them. Thus, a lot of them believe both that the vaccines cause autism and also that they’re being used to microchip people. Unless the theory is that it’s the microchips that cause autism? I kinda want to see the overlap in the crosstabs, I’m expecting to see a lot of it.
Thus, my best guess is that about half the ‘hesitant’ are getable through some combination of things getting bad and us picking the low hanging fruit like approving the vaccines, and the other half likely require stronger stuff.
Once and Future Lockdown
Could it happen again? Janet Yellen thinks so.
Nate Silver mostly disagrees.
Nate’s mistake here is to act as if a cost-benefit ratio is all that relevant to how decisions are made on Covid. Somehow we have decided that ‘forcing’ people to take the Covid vaccine is unacceptable, and that’s that. So our choices are instead forcibly disrupting people’s lives in the hopes that it helps, or not doing that. If things get bad enough, it makes perfect sense that we’d potentially see lockdowns but not vaccine mandates, and that those lockdowns likely won’t make exceptions for vaccination, because we’ve also made it unacceptable to check someone’s vaccination status in most contexts and places.
Where I think Yellen is clearly wrong is in expecting the places with low vaccination rates to be the ones that lock down. It’s almost certainly the opposite. If lockdowns happen, they will happen in the places with relatively high vaccination rates. Not the highest like Vermont, since they’ll have no need for it (probably), but in the various blue states that time and again have gone overboard with prevention. There’s zero appetite for locking down red states.
I’d hope there was zero appetite for locking down anywhere, but I am growing more worried about this possibility. It’s really stupid, because it wouldn’t work. Even if it did suppress Covid entirely in the local area, the moment you stop it comes back, so what’s the point? When will things change? Are you going to keep this up for years?
I do see signs that there’s support for doing exactly that. Some of this is ‘avoid blame on a two week time horizon’ where the fact that the problem never goes away isn’t relevant, but some people really do support permanent ending of life as we know it. I don’t understand why they are so cool with this, it seems like the later stages of a Persona game or something, but it is what it is.
Meanwhile, Biden tells us our young children will be wearing masks, whether they like it or not:
I am getting really tired of this malarkey line about not interfering with ‘scientists’ as if they’re all identical clones who reach all the Officially Scientifically Correct conclusions, and thus one doesn’t have to take responsibility for decisions if you can cite one. You did it, sir. You.
Similarly, Washington Post reports that the Biden administration is debating urging a return to masking for the vaccinated. It would ‘have to come from the CDC’ but they’ve ‘taken a hands off approach to avoid interfering.’
So Biden says this:
…and pretends that this isn’t him giving the CDC an order.
Presumably, this is all an attempt to avoid blameworthiness for decisions that are sure to be unpopular, rather than a bizarrely wrong theory of the scientific nature of public policy.
In Other News
Your periodic reminder that Gain of Function research needs to stop and this is a major test of our civilizational adequacy:
Alternatively, someone could come up with math that could possibly justify these kinds of risks. If someone has done so, I see no signs of that.
Whereas you know what we’re not funding much, even now? Pandemic preparedness.
You’d think they’d wait for the current crisis to be over before failing to prepare for the next one. That is, you’d think that if you hadn’t been paying attention.
Eliezer also had another interesting thought:
As several people pointed out, as a legal matter you can’t actually ask such questions, so we’d put it in the pile of all the things you technically aren’t allowed to ask or consider that we all know employers ask about and consider all the time.
Alex Tabbarok reviews The Nightmare Scenario. Report makes clear the book contains a lot of good concrete information, but nothing that would meaningfully change our model of what happened. Yes, that means all the things mentioned in the review were already in the model. I might read it anyway at some point, but my guess is I will decide that I won’t because I don’t have to.
Update on the Novavax vaccine.
In a strange display of the right thing being done, Taiwan approves a vaccine purely based on immunological data.
While I am not looking into such questions in general Because Of Reasons, I did see this notice that one of the Ivermectin studies was withdrawn due to ‘ethical concerns.’ Where the ‘ethical concerns’ in question appear to be ‘massive fundamental discrepancies in the data’ which is a nice way of saying ‘complete and utter fraud.’ Figured I’d pass it along. How this impacts your model of the situation otherwise is up to you – among other things, I didn’t check to see how fundamental this evidence was to the case.
Los Angeles resumes its mask mandate, including for the vaccinated. If it’s back now it’s hard to see what could happen any time soon to get it lifted. If you don’t like it, you may, like many others before you, finally want to look for another place to live.
Las Vegas brings back its indoor mask mandate as well. Las Vegas seems like the place maximally in need of such a mandate, given all the travel and all the poorly ventilated completely enclosed spaces designed to trap you inside for indefinite periods. In that one case I at least kinda get it.
You know who isn’t masking? Democratic politicians fleeing Texas on a private jet in order to deny a quorum and prevent the state government from functioning. Three of whom then tested positive for Covid.
(There was previously a thread here about people in the UK facing legal trouble for going outside to remote locations ‘to avoid detection’ but it appears likely it was fabricated.)
Australia enters this week’s Sacrifices to the Gods competition, to crack down on those who put us all in danger:
Via MR, some notes on Peru, and they may have won the Sacrifice to the Gods competition on sheer sticktoitness. It’s impressive stuff. Other non-Covid stuff after is wild too.
Also in the UK, escalating quickly: Not only First Doses First, Second Doses Too Early Actively Dangerous and Scandalous:
California’s entry isn’t going to get it done, but it’s still quite the display of self-harm:
So her friend has Covid, and is being told to travel back to California so she can get tested locally, because out-of-state tests don’t count for tracking purposes. Explain again how our policies are trying to contain this virus.
MR looks at a report on Oaxcana’s (in Mexico) precautions for travelers. Everything except the masks is clearly useless sacrifices. Tyler speculates that this makes it easier to otherwise be open. That’s possible but my presumption as per usual is that nothing as sensible as that is going on here.
Everything that is not compulsory is forbidden. Everything that is not forbidden is compulsory.
Our Covid prevention efforts, all of them, well OK most of them, in one tweet, including the part where the explanation for the beds probably isn’t true and they’re just a terrible design for no real reason:
One person with a cameo tests positive, and that’s it. Show’s done. Them’s the rules.
Finally, if this is his official platform and he confirms he wants to build more apartments, I hereby endorse Nate Silver to be the next Mayor of New York.