Chronicle of a parent who finally lost it when their child’s school closed for ten days due to two Covid cases… for a fifth time. New York City is finally changing that rule. It was even more absurd than it sounds...
I am confused about why this is bad. It seems like an all-around excellent rule: if you see cases and you know where they came from, then just shut down the places where they came from - i.e. affected classrooms and close contacts. If you see cases and you don't know where they came from, especially after explicitly attempting to trace, then that should set off giant wailing alarm bells and a voice on a loudspeaker yelling "ALERT! Hazardous unknown detected!". Shutting down the whole school for ten days sounds like exactly the right move, when there are multiple cases popping up and we don't know why.
As an added bonus, this policy should both incentivize cooperation with contact tracing (at least for anyone looking to keep the school open) and naturally lead schools to close more often as background cases in the general population rise. And these "bonuses" are not coincidental - they both involve the sort of "unknowns" which we want to detect, namely multiple measured cases for reasons other than traceable interactions.
Agreed. In addition, the quoted article is summarizing the policy incorrectly it seems: They write that the school will be closed when there is no evidence of in-school transmission, but that is wrong: if contact tracers find the source as outside of the school, the school will (presumably) not be closed.
If the school shuts down the kids will just go back to the street. We do not send kids back into school when we observe transmission from kids being out of school. The evidence from Emily Oster suggest that there isn't much difference in transmission.
Also, I would argue that a small amount of transmission is worth educating our children, especially with 70-80% of the vulnerable vaccinated. Overall dividing life years lost by transmissions comes to 2 weeks per confirmed infections, so call that the base cost. Reduce it by 75% for targeted vaccination and each case is costing ~3 days of a persons life. And the student infections are the least dangerous kind. I could go either way on it if the alternative were no transmission. Since the alternative is about the same transmission rate but somewhere else, I say keep the schools open.
OTOH, the incentive argument is much stronger. Maybe the collective punishment forces the school to internalize the cost of transmission, leading to a pareto improving safe-school equilibrium.
I need empathetic support in screaming against yet another dumbass decision (6 "strange" blood clots events... in 7 million shots).
https://www.nytimes.com/2021/04/13/us/politics/johnson-johnson-vaccine-blood-clots-fda-cdc.html
No sane major corporation is going to have a batch of 15 million doses and not test it to see if it is the thing it was meant to be before shipping it out, and having something in there that wasn’t supposed to be there should get found many times over by the tests they’d run in all worlds. Ordinary corporate reputation and liability are more than enough to motivate catching this error.
https://pubmed.ncbi.nlm.nih.gov/24785997/
A company bought by Bayer shipped out many doses of blood products that they knew were contaminated with HIV.
To be fair, they didn't know which doses where contaminated at the time and there was no test to determine which doses were contaminated.
I'm curious about what the state of evidence around long covid is now, and especially how protective vaccines are against it. I imagine there still isn't much data about it yet though.
I work at my county's health department helping with the vaccination process and I can confirm that you are scheduled for two weeks out exactly when your first shot is done. If you miss that date or have to reschedule you are put on a waiting list for a different date in time, I don't have access to the list, but I also assume it's scheduled for you again with the hopes things will just work out.
I take inbound calls sometimes and many people are worried if they cancel they won't ever get, or since it's been longer than 2 weeks "something" would happen where they wouldn't get full immunity. If you've been reading these posts for a while I don't think it should be surprising that lay people take the knowledge they are given on the covid issue without question. I think for most cases that's reasonable and tends to work well.
Our department is greatly over worked as well. when we register people in our system we try to put their preferred contact information as email since that is sent out automatically when that person is in the available age / priority group. If they sent their preferred method as call they might not ever get a call telling them they can schedule for appointments since we have very few staff (I haven't met any) who do outbound calls or have the time to do them. This has a major impact in our elderly community as they usually can't figure out technology as well as younger people, and the vaccination registration slots will be filled by the people that can work computers.
I have had many times older people call our vaccination line and wonder why they haven't been called to be scheduled after signing up so long ago, only to see they have been sent an email months ago but nobody could call them to tell them to register. When I was working at the vaccine clinic earlier today one guy wondered in, said he never got a confirmation time since nobody called but it had been two weeks since his first dose, sure enough he was scheduled for today and we got him his second dose.
I'm not high enough to know any more logistics or bottleneck issues other than that, but like most massive projects it's chaotic, with information changing rapidly, and little optimizations and setbacks happening all the time. To leave this post on a hopeful note, if they show up to our clinic and are in an eligible group, if we have shots left to give we get them registered and get them the shot that day. We also push through the spouses of the people there getting vaccinated as well. Most other vaccine workers like me try to push through as many people as we can as painlessly as possible, fighting the grinding wheels of bureaucracy as much as we can. We understand we are here to vaccinate, not pencil push, little formalities are easily overlooked. I hope it's the same for clinics in other parts of the state's as well.
Have you or anybody else sensibly written about the P1 variant in Manaus? Despite a prior infection rate of ca. 75% in January, Manaus not only experienced a surge in new infections, but also a record high in hospitalizations. This is evidence against the usual assertion that T-cell immunity will provide enough protection against new variants that we will not have to worry about Covid-19 anymore once 70% are vaccinated.
https://www.thelancet.com/article/S0140-6736(21)00183-5/fulltext
My impression at the moment is that all the claims that P1 causes loads of reinfections depend on this one study of Manaus blood donors that found 75% prior infection rate. Other lines of evidence (e.g. testing neutralising antibodies) suggest that P1 is more like the UK variant B1.1.7 - more infectious and more lethal but less immune escape than the South African B1.351 variant.
Now one of these viewpoints must be wrong, and I'm inclined to believe it's the blood donor study that's wrong. Beyond usual worries that blood donors might not be a random sample, apparently people donating blood were also told their COVID-19 antibody status, so people who thought they had been infected might have been incentivised to donate blood. There's also a different study ( SARS-CoV-2 antibody prevalence in Brazil: results from two successive nationwide serological household surveys ) which finds 14% prevalence in June, compared to 66% from the blood donor study.
Caveat: I haven't been following this super closely so may well have missed some relevant results. I also haven't looked into the credibility of the second prevalence study at all.
“What’s scary is when I try to put a probability on ‘this turns into a broader thing that outlives Covid and people have to show the computer has them in good standing to get on a train’ or something like that. I still think it’s a super low probability thing, maybe 2% (it’s a Fermi answer, but a considered one), but that’s 2% of a really, really bad outcome.”
I’m sorry, but the 2% strikes me as pure optimism. If the government gets vaccine passports approved for anything, the probability is very high that we’re stuck with them for the long haul, and that use will gradually expand over time from slippery slope effects.
As a comparison, think about all the civil liberties lost after 9/11 and how you never got most of them back. Eliezer Yudkowski wrote that it was a vast underestimate to think that the overreaction to 9/11 would be ten times worse than the event itself. Every bias that caused the overreaction to terrorism is also present and causing the overreaction to Covid. Vaccine passports are part of that overreaction!
Think about how governments learned to shout ‘terrorism!’ any time they wanted more power and how those powers always ended up being used against more than just terrorists. In the US you guys had the NSA snooping on everything and everyone, terrorists or no. Here in the UK one very sinister example is the 2001 Anti-Terrorist Act which our then-government solemnly promised would only be used against terrorists. Within a few years it was being used to seize assets from Icelandic banks for the crime of being inconveniently bankrupt. You simply cannot trust governments to only use their new powers against the original target. Once you add a tool to their toolbox, that tool gets used.
Now really think about what it would take to be the politician or bureaucrat that tried to scrap vaccine passports. You’re up against fear of blame and the Copenhagen interpretation of ethics: whoever makes that decision is at risk of being blamed for every person who ever gets sick again. They will be demonised by the other side as pro-virus. Then there’s simple status quo bias: once the passports exist scrapping them then becomes a change in the status quo and subject to inertia, akrasia, and the difficulty of coming to consensus.
I hope you now understand why I am fundamentally opposed to vaccine passports. I hope I have persuaded you too. This is a terrible, dangerous idea, and the time to stop them is before they become the status quo.
It seems like there is new evidence of significant risk of blood clots associated with the AstraZenica vaccine for young women.
That story references but does not cite these studies from the New England Journal of Medicine:
So it seems like there is significant risk associated with the AstraZenica vaccine for certain age groups, and that it may make sense to avoid for those people.
Young women have significant risk of blood clots because the pill has significant risk of blood clots and they are the demographic for the pill.
The fact that we see the cases in that group suggests that it's not about "certain age groups" but taking the pill.
Speaking about "certain age groups" might be the result of too much political correctness getting in the way.
These blood clots are unusual and triggered by immune-mediated platelet activation, and happening at higher rate than the base population in those subpopulations. It's real and not the pill.
It's also lower than the risk of the pill.
Yup. High stakes free rider problem, in which we are comparing individual risk to collective benefit. And the moral calculus is a moving target.
Then the week afterwards, the world learned that Emergent had put ingredients for the AstraZeneca vaccine into a batch of Johnson & Johnson vaccine, running the entire batch of 15 million doses.
Did you mean "ruining"?
Vaccinations were not prioritized perfectly, but they were prioritized well, and they protect even better against death than infection.
I'd be very interested in hearing (from Zvi or anyone else) more about where you stand on the extent to which vaccinations protect against death. Death is the main thing I'm trying to avoid. If we were confident enough that it protected against death enough, I would up my risk tolerance.
Given the numbers COVID-19 vaccines are less effective against asymptomatic infections then they are against symptomatic infections. We also see them to be more effective against hospitalization then against symptomatic infections.
Given that death is at the tail, they are likely more protective against death then asymptomatic or symptomatic infections.
The effect they have on long Covid is less clear. Long Covid won't kill you immediately but can plausibly cost you a few years of lifespan.
Can you please provide a link to somewhere explaining why links to unvaccinated are higher than they appear.
My assumption is that the risk I take is proportional to the number of people which can transmit Covid that I meet. If vaccinated people still present the same risk of transmitting Covid to unvaccinated people and do not get tested, then your number makes sens. But it does not seem that it is what you have in mind.
I also understand that some people takes more risk as they know that a lot of people nearby are vaccinated. Or simply because the government restrictions changed, forcing them to go back to work even without vaccine.
If we want to track whether anything makes the virus more dangerous than it used to be, I understand that statisticians need to take the percentage of vaccinated people into account to measure the actual risk of transmission from an unvaccinated person with Covid to another unvaccinated person. So, clearly, if a new variant arrives and get dominant in my town/lander, the update I need to make about this variant is greater than the usual update I need to make about new variant. But this statement do not seem to be as important and far-reaching than the statement you made, so I suppose I missed something. Any help to understand what I missed would be greatly appreciated
Did you have a look at the https://covidtracker.fr/covidtracker-world/ project ? It does not give the amount of details you used to have for the USA (as it is a French site) but it seems to do what you want country by country.
I’ve been travelling to New York City once again, and it’s been a busy week, including putting in bids on multiple different apartments. Developments are ongoing, so I’ve been even busier than usual and it’s likely some stuff has slipped through the cracks.
The overall situation seems unchanged. As people take more risks and the new strains dominate, we’ve settled into about a 10% week over week growth in positive rates, but due to vaccinations death rates continue to decline. That means that one’s risk as an unvaccinated person continues to rise, even as risk on a population level goes down. With everyone eligible now or at least soon, I’d urge once again for everyone who isn’t yet vaccinated to schedule an appointment as soon as possible.
Many places that have less robust vaccination efforts than America are seeing record high case numbers and hospitalization numbers, as the new strains overwhelm efforts that were previously calibrated to let things stabilize. Things are quite bad out there in many countries. Check your local situation, and act accordingly.
Vaccination rates have stalled out in America, but at 3 million shots a day, which will still get us there pretty soon. Unless something unexpectedly makes our situation worse, we should reach the tipping point on vaccinations within a month or two, at most within three, after which we see a steady and accelerating improvement across the board.
Let’s run the numbers.
The Numbers
Predictions
Prediction from last week: Positivity rate of 5.3% (up 0.4%) and deaths are unchanged.
Result (on Friday):
Deaths falling a lot indicates that last week’s failure to drop was a measurement error, and the numbers from Wikipedia were more accurate. On reflection, I should have realized this and made a better prediction. The positive test rate number matches my intuition.
I notice I am confused by the continuing decline in test counts. It’s faster than the rate of new vaccinations, and the number of cases isn’t declining. I haven’t seen a good explanation. Seems like an important piece of the puzzle.
Prediction for next week: Positivity rate of 5.9% (up 0.4%) and deaths decline by 8%.
Deaths
Oklahoma reported 1,716 deaths due to finding previously uncounted ones. I’m calling that 100 deaths from this week based on their previous weeks, and assuming the rest were in the past.
Cases may have stopped falling several weeks ago, but deaths continue to improve each week across the board, with improvement even in the Midwest. Vaccinations were not prioritized perfectly, but they were prioritized well, and they protect even better against death than infection. It makes sense that deaths continue to decline, and I again affirm that my prediction on this last week was bad.
Cases
Vaccinations
Progress on the rate of vaccination seems to have stalled out for now, which is disappointing. Still, three million shots per day is pretty good, and one third of the population has had its first dose.
Vaccine eligibility map is complete. At this point, most of the light blue states (not California, Washington or Illinois) have open eligibility, as do all the green ones, so within the week only six states will be left, and everyone’s agreed to finish it by May 1 at the latest. Since this was created, New Jersey moved up a few weeks, so it’s only Oregon and Hawaii waiting out the clock.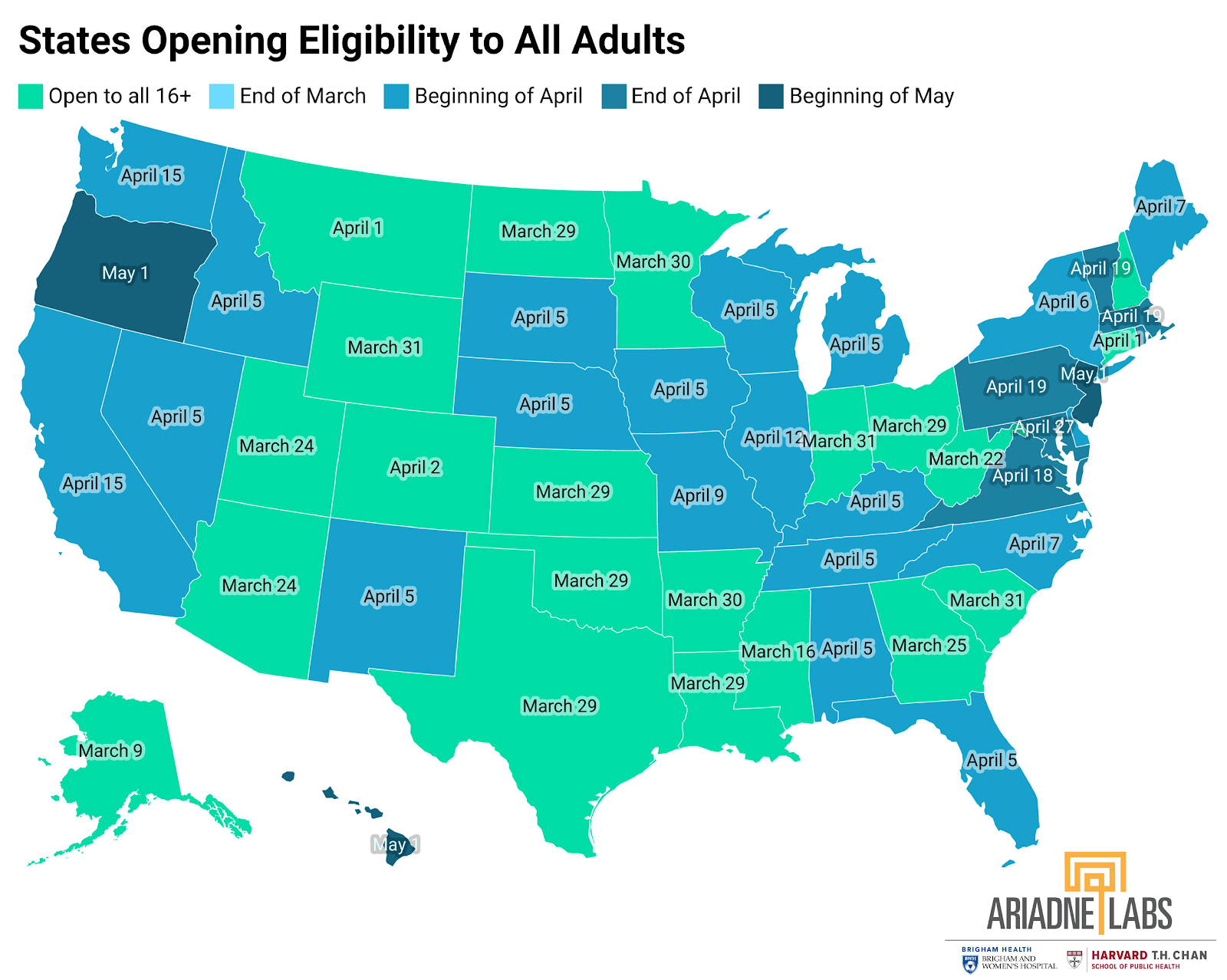
Vaccine Passport Hype
There was a lot of vibrant discussion of vaccine passports in the comments, both on the blog and on the crosspost at LessWrong. Topics ranged from the technical feasibility of various ways to conserve privacy while ensuring accuracy, to various strong opinions about how we should operate in general once vaccinations are freely available.
As many pointed out, the conflict between security and privacy is difficult in practice. Usually we fail at both, such as a driver’s license to buy alcohol, where it’s not that difficult to fake and also reveals who you are, although without any automatic record. Having a QR code unique to the individual means some “they” could track the QR code, if desired. Having a one-time QR code continuously generated wouldn’t work with people without phones and might generally be tricky. And of course, if they can’t tell who you are claiming to be, there’s nothing stopping you from using someone else’s QR code by borrowing their phone or what not.
As usual, if we have a system that effectively requires you to either get vaccinated or have a willingness to use an app to fool the system (i.e. lie about your status) that is a subsidy to the dishonest. That can be difficult to avoid.
Overall, I think I’m fine with a system that’s relatively easy to fool at any given time for those making an effort, in order to preserve privacy. There’s still a record of who was and wasn’t vaccinated, so when it matters enough, records can still be kept and cross-checked. It also lets those running venues, from restaurants to stadiums, avoid blameworthiness and get on with the show. Everyone shows their passports, and life can resume. If a few people aren’t vaccinated, they might infect each other, but if they’re making an effort to get in via fraud then I feel fine with that being the consequence.
My guess is such fraud will be rare if it’s even a relatively trivial inconvenience. It’s easier to get the vaccine, even if the fraud isn’t that difficult. I already know of several concrete examples from this past week. For example, I got my first post-vaccination haircut, and the (young) barber said she was going to get vaccinated in order to be allowed to do stuff. I pointed out that it also would be nice not to get Covid-19, and despite the other barber pointing out he still didn’t have his sense of smell back after catching it, she didn’t seem to notice that the vaccine might have a health benefit to her. And yet, she (quite reasonably) was eager to get it the moment she’s eligible.
What I see playing out so far is exactly what one would hope, which is that the expectation of needing to be vaccinated is causing people to get vaccinated, without any need to actually impose meaningful restrictions. If that works, then we won’t have to.
Others disagree, including large states. Texas is banning the use of vaccination passports (WaPo). Florida has taken a similar position. I am curious to see if this results in situations where their venues are often not at full capacity for longer than in other places, despite starting out ahead of the curve, or if the culture that disdains the passports also allows life to return to normal without them and shrugs at the consequences. That shrug will hopefully be reasonable not that long from now.
I missed at least one good objection. From the comments:
If people depend on a vaccine passport, then anyone who can take that passport away will be tempted to use or leverage that power. Would the government take the passport away from you if there’s a warrant out for your arrest? If you have unpaid parking tickets? If you attend a protest?
Or, you could raise the more generalized version of this objection. Also from the comments:
Let’s generalize the argument, which is a strong one. The proposal the vaccine passport is really making is to gate freedom of movement with a government document on your phone. This is ‘papers, please’ everywhere, with GPS tracking and check-in logging plausibly attached. It isn’t simply a question of whether the government will abuse the records to track people. It’s a question of what will happen once it realizes that it can change the requirements to get papers, or what information is revealed by those papers. Historically this all ends quite poorly, and one should quote Benjamin Franklin.
I should have taken this objection seriously enough to list it and respond to it, and that I didn’t do so worries me. It really should be a 101-style extrapolation, even if there are good reasons not to expect such outcomes here. At a minimum, it definitely does lower the bar for similar future systems that are more likely to be abused – accelerate such trends, as Craken puts it.
What’s scary is when I try to put a probability on ‘this turns into a broader thing that outlives Covid and people have to show the computer has them in good standing to get on a train’ or something like that. I still think it’s a super low probability thing, maybe 2% (it’s a Fermi answer, but a considered one), but that’s 2% of a really, really bad outcome. It’s not obvious one should take those odds. The argument that convinced me is that in the 2% of worlds where this happens, I think mostly it was going to happen anyway within a reasonably short time frame, one way or another.
So on reflection I think this a real downside, but that ‘give everyone the information that matters and let people do what they want with it’ is still the right attitude. Your vaccination status simply isn’t a private concern, it matters to those around you. The alternative to a passport is people either literally laminating their vaccine cards (hence CNN running with the headline ‘things to do before you laminate your vaccine card’) and using a super-easy-to-fool system, or banning people from asking about vaccine status, and those alternatives seem far worse.
This also relates to this other instinct, which I also understand:
If I felt this was centrally government coercion, I’d have a different view. Instead, I view this as providing for the flow of necessary information to let us all make informed decisions, which in turn enables behavior that would otherwise effectively be shut down entirely by coercion and/or by health risks, and the worry is that future action will transform the passports from vaccination information flow into a more general case of the government coercion thing.
Risk to the Unvaccinated
I haven’t said this explicitly in a while, so it’s worth saying it again: If you are not vaccinated, the current level of risk out there is much higher than the graphs and charts naively imply. On top of that, the cost of getting Covid now is much higher than it was earlier, both because the new dominant strain is deadlier, and also because the main benefit of getting infected – that you can’t get infected again – no longer matters much since you’ll have vaccine access soon either way and things aren’t so bad out there that prevention is hopeless. You won’t even be able to skip the vaccine, due to people requiring it (plus it’s a good idea anyway, since the cost is trivial).
Not only have we vaccinated over a quarter of the population, and given one dose to over a third of the population, we’ve done so with an emphasis on those most at risk.
That means that if you’re in the remaining two thirds, not only is your risk a third higher than it looks (e.g. almost all the infections will happen to unvaccinated people) but also the risk of death is more than double what it appears, as those at risk have largely been vaccinated early.
Thus, if you have not yet been vaccinated, you need to treat things as much more dangerous, relative to the past, than the numbers indicate. Over time, this effect will get larger.
This Atlantic article by Katherine Wu points out the phenomenon of people seeing vaccinated people going around doing things, and various gatherings happening, and the resulting temptation to take more risks and feel as if things are safer now. They’re a lot safer than they were in December, but in many places and in America overall they’re much less safe than they were any time before October. Don’t lose sight of that.
Interacting with vaccinated people still has very little risk involved, but using the vaccinated as an excuse to do things involving other unvaccinated people, that you wouldn’t have done in a situation like the one in October, is a trap to be careful about.
Did the FDA Get One Right?
Two weeks ago, I noted that the FDA hadn’t even approved Emergent to make the J&J vaccinate, and that this was holding up production to the extent that it looked like all the doses actually being using ingredients from abroad instead:
Then the week afterwards, the world learned that Emergent had put ingredients for the AstraZeneca vaccine into a batch of Johnson & Johnson vaccine, running the entire batch of 15 million doses. That’s a true disaster, enough to set back the overall American vaccine effort by over a week. The mind boggles at how many lives we’ll lose and how much economic value was lost, including being later to start exporting overseas.
I didn’t connect these two events at the time in my head, so I didn’t mention it, and deservedly got this comment challenging that:
It’s hard to argue against the claim that if someone refuses to give someone else approval to do something, and the next week they massively screw up doing it, and also it turns out they’ve had similar (if I presume less dramatic) issues in the past, that the refusal to approve has to look at least somewhat reasonable. One needs to notice this, and update, or if not updating then clarify why that shouldn’t be the case.
At a minimum, this should have been explicitly noticed.
One incomplete but important question to ask is, in this particular case, what did the FDA’s intervention change?
Then we can ask the more important question of expected value. What does this type of intervention change in expectation, in general, and at what cost?
Let’s start with the obvious. Did the FDA’s refusal to give approval to Emergent prevent a disaster? Would we have otherwise been looking at giving out 15 million contaminated doses, likely useless and potentially dangerous?
If so, then this is strong evidence that the FDA being picky about who can get manufacturing approval has high value, whether or not it justifies the costs involved, and that would transfer a non-zero amount to other types of FDA approvals as well. The whole idea is to guard against disasters.
I have not seen any details on how the error was noticed, so we can’t be certain of the counterfactual, but my very very strong prior is that this error gets caught in all worlds. The composition of the batch was wrong. No sane major corporation is going to have a batch of 15 million doses and not test it to see if it is the thing it was meant to be before shipping it out, and having something in there that wasn’t supposed to be there should get found many times over by the tests they’d run in all worlds. Ordinary corporate reputation and liability are more than enough to motivate catching this error.
My model says that’s not how the FDA is even trying to prevent this mistake when it withholds approval. The FDA’s strategy for withholding approval is to force Johnson & Johnson to use a better manufacturer using better procedures. The failure to get approval, based on the FDA noticing that Emergent does not know what it is doing, is a heavy incentive for J&J to find another partner here. What is interesting is that this didn’t happen.
That’s the part that’s still baffling me. If Emergent had a bunch of violations already, and was going to have trouble getting approved slash hadn’t already been approved, why did J&J use them rather than someone else? My understanding is that J&J’s vaccine uses relatively well-established manufacturing procedures, so they had plenty of options especially given their lead time and deep pockets, and also there wasn’t much risk that key knowledge would leak out in this fashion. That also implies of course that they should have been using multiple factories to make a lot more vaccine doses faster, although there could be another limiting factor somewhere on the ingredient list.
The benefit of the whole FDA system comes when corporations look ahead to the approval process, notice they won’t get approved unless they did things right, and then people do their jobs right in the first place, or it comes when the FDA notices something bad that wouldn’t have otherwise been noticed and stopped, and stops it. The second mechanism is important to the extent it happens.
The question here is why that first mechanism, which is supposed to be how you stop this disaster, failed. And by implication, how often this mechanism silently prevents disasters in other situations, that would otherwise happen. It’s a thankless job to prevent disasters that, if you succeed, no one knows were ever an issue. That’s the dog that didn’t bark. I don’t think that it happens often, because I think there are lots of other robust checks that would work instead, but it’s reasonable to disagree with that.
The blame in this particular case looks like it falls on J&J (and of course on Emergent), to the extent that I’d want to downgrade my view of their prospects and stock on the basis of J&J likely being less good at what they do than we thought. J&J knew full well Emergent was a risky choice here, without the necessary experience, and used them anyway. If anything, it seems more like the FDA ended up effectively forcing J&J’s hand because regulation made it much harder to build a new plant or spin up a new partnership, which would have required a whole new set of approvals across the board. If they didn’t have those obligations, they would have had other options.
By tying everyone’s hands and delaying things across the board, and generally constraining the range of possible actions and actors, my guess is the FDA made this disaster more likely. They definitely made it more of a problem, because without them we’d be way ahead of the current schedule for vaccine production across the board. Certainly ‘catching this’ does not justify the red tape they’ve thrown over vaccines and also everything else.
The FDA did, to its credit, provide strong evidence that its decision to withhold approvals was based on a legitimate real world consideration, and that in general, however slow and cumbersome what it does might be, it at least does provide some amount of quality checks and safety standards. That’s much better than not doing that. They’re a sane regulator, responding to their incentives, which put very little weight on production they prevent or innovation they stifle, the time and money and lives lost through inaction, and almost all focus on avoiding disasters due to action, or avoiding being blameworthy for any disasters due to action that aren’t prevented. Within that framework, one could plausibly argue they did their jobs quite well here.
The goal is to change the incentives and the job.
One can also ask how exactly we got into this mess, since Emergent is so obviously a terrible choice on so many levels, and the answer is that they’re a government contractor hired explicitly to handle exactly this problem, except they chose a company with a long history of problems and which the FDA refused (with reasonable justifications) to certify:
It was a great idea to pay to have capacity always at the ready. The problem was that this was a contract awarded on the basis of politics and power, rather than by the market, and thus people whose focus was on winning contracts via political power games, and which not coincidentally didn’t have that much to do all day because no one else was that eager to hire them, beat out the places that would have been capable of actually doing the job.
This makes J&J’s fate somewhat more understandable. They chose a terrible partner, but it wasn’t entirely their choice. Once again, the free market fails due to lack of a free market, requiring intervention from regulators.
In Other News
England offers free twice-a-week at-home tests to actual everyone. It’s about time. A day late to be sure, but all the pounds are there.
Meanwhile, we’re a little behind that, but at least we’ve… legalized Abbott to do home testing? (Source)
Kai compares what happened now to the response to AIDS.
Starting to see frequent posts on Twitter about available vaccine appointments. For example, here was Sam Black, although that one’s in the past. Here’s another from LA, presumably also expired by now. The bottom line is, keep an eye out for such opportunities if you or anyone you know has had trouble finding an appointment, or would like an earlier one.
Our government allocates life-saving medicine explicitly on the basis of the racial identity of your household. Then it restricts what people’s movement and what they can do if they haven’t yet had access to that medicine.
Chronicle of a parent who finally lost it when their child’s school closed for ten days due to two Covid cases… for a fifth time. New York City is finally changing that rule. It was even more absurd than it sounds:
From the perspective of actual people leading physical lives, this is indeed nuts. From a blameworthiness perspective, and a ‘state of grace/purity’ versus ‘state of sin/contamination’ perspective, though, and a very explicit ‘if I can say it’s keeping kids safe I don’t have to care whether it makes any sense or drives people crazy and disrupts their lives’ perspective (that was the first reply to the Tweet announcing the story), it makes perfect sense.
Efforts to promote First Doses First continue, remain obviously correct, remain doomed to failure. I don’t see any way to turn this one around at this point. We are requiring full vaccination to engage in everyday life, so people aren’t going to accept going around half-vaccinated even if it’s 90% as good, so long as they’re told to treat it as 0% as good.
Gentle reminder that if you book your appointment for a given day, you’d better be ready to get the second dose exactly the right number of weeks later to the minute, or you’ll need to actively reschedule at a minimum:
Your periodic reminder department:
I think Eliezer is flat out correct here that it’s dirt cheap to build out what we might call ‘generic mRNA vaccine capacity’ and that even if the pandemic was over we should be doing enough of that to vaccinate everyone, except I’d say the USA should be planning to make enough for the whole world, not only Americans, because the payoffs here are so ridiculous. Instead, we aren’t even doing this for the current pandemic. The footnote on never even investigating far-UV light properly is also a good periodic reminder.
Our lockdown rules being applied differently depending on which groups and activities are favored by politics and power is the default, not an exception.
We repeat, suicides were actually down last year, rather than up. Your model needs to account for this.
We see extra deaths from heart disease, Alzheimer’s disease, diabetes and stroke, and in general about 140k extra deaths on net that aren’t listed as being directly from Covid-19. Some of those are likely Covid-19 deaths that got misidentified. Some others are likely due to people not getting any exercise or change of scenery. What we don’t see are suicides.
CDC finally starts getting explicit on surfaces not being much of an issue. Still a lot of ‘it depends’ and ‘we don’t know anything about anything’ but the bolded part is bolded:
Tyler Cowen and Russ Roberts podcast revisiting the state of the pandemic. Self-recommending and as good as you’d expect if you like this kind of podcast conversation. Cafe Hayek responds, arguing that Covid response has been far more damaging to social cohesion than it would have been to let things play out. Tyler in turn responds that this wasn’t an option, because once things got worse the lockdowns would have happened regardless, from a worse place, and been more severe. I’m with Tyler here, the alternative to lockdowns that works is to do more earlier, the public choice of letting Covid mostly play out was never going to do anything but backfire. There are still some clear examples in the response post of utterly crazy policies in the name of prevention, of course, as I often point out.
Health care provision across state lines, to-go cocktails and other purely good deregulations that might stick around (WSJ via MR).
Post on the option to use IP suspensions to solve the vaccine shortage, and alternative ways to get production to go up. That seems like a disastrous road to go down, and if formal IP was the issue we could simply buy the companies out, which the post points out is the correct play here, plus the post also points out that mere suspensions wouldn’t actually work, because (among several other reasons) the IP that matters is not in the patents. So Moderna won’t enforce its patents but that doesn’t mean anyone knows how to make its vaccine, and those secrets are valuable to Moderna for future products so they won’t share. Of course, we could buy them out of that too if we were sane, it’s worth it, but there’s no willingness to do so. Also of course, the simple play is to offer to pay a lot more money to get vaccine doses, and let them work out the rest, but that’s crazy talk.
Zaynep thread about claims that places have reached herd immunity.
Finally, this seems very right, and it’s important once you’re fully vaccinated to remember to live your life once again: