It actually seems to me that daycares would be a natural setting to trial the new consumer far-UVC, air purifiers, good HEPA filters, or mandatory daily flu/COVID testing for the kids. You could potentially have a rule that kids who come in sick get semi-quarantined (only contact is with masked adults/sibs, they must wear a mask). That's a setting where it might really make a noticeable difference and where you don't have to convince an institution to retrofit a whole large building.
Apparently an air purifier cut sick days by a 3rd in Helsinki.
There's also an ongoing trial called CLAIRE on using HEPA filters in schools.
https://clinicaltrials.gov/study/NCT07479420
A re-analysis of data from the 1940s found far-UVC dramatically reduced child absenteesism due to respiratory illness
Far-UVC has been shown to be extremely effective in reducing pathogen load in the air.
https://pubmed.ncbi.nlm.nih.gov/35322064/
Maybe it's time for somebody to open an aggressively sanitary daycare.
I agree and have thought that a daycare that leans into these measures would be great. The economic benefit alone of minimizing sick days that parents must take to care for sick children would be huge.
One small comment about the Ryan C. W. (2023) article on the 1940s data is that it is referencing upper room Germicidal Ultraviolet Light (GUV) which is about 254nm light and not far-UVC which is 222nm. GUV could be used in a daycare setting in the modern day, however, it would require specific infrastructure that far-UVC probably would not need (the CDC mentions a minimum of 8 foot ceilings).
Another site that has some good far-UVC resources is @jefftk's site https://www.faruvc.org/.
Sure it is! You just need to use a powered version. https://pekesafety.com/collections/powered-air-purifying-respirators
Hard to tell because I can't find a news article linking the study, but I think https://www.sciencedirect.com/science/article/pii/S2950362024000043 is the Helskinki study.
we used portable air cleaners in two day care units (A and B, number of children participating in the study n = 43) and compared infection incidents between the two intervention units to the rest of the units in city of Helsinki (n = 607). ... At day care centre A the average reduction was 60% (range 52% - 88%) and at day care centre B 53% (range 14% - 59%). ... On average, the parents were absent from work due to child’s illness in reference day care centers for 5.53 days and 3.77 days in intervention day care centers during the study period (p=0.009). In relative terms the reduction was approximately 32%.
I agree that children getting diseases at daycare is a significant problem. You didn't mention it, but this also means parents get sick more via their kids.
Many arguments about daycare are motivated reasoning because it's personally necessary, or because of ideology: "enabling more women in the workforce is good and therefore things that enable that can't be bad".
Or "fewer people would have babies without day care and therefore things that enable that can't be bad."
The strongest motivated reasoning comes from cases where you feel obligated to do something. If it's locked in, you may as well cope about it, rather than continuing to negatively think about it.
The few recent times I‘ve gotten sick it’s been when I visited my dad’s kids. I didn’t think about it until now, but I’m going to see if I can meet them in outdoor gatherings instead.
I remember looking into exactly this question when my wife and I were looking into pros and cons of daycare. One thing that I think the analysis here misses is that this is generally worst for the first 1 or 2 years, and then much less so. I don't remember exactly what studies I was looking at back when I was researching this, but asking Claude just now "Is there a study that looks at the frequency of child illnesses by year after first enrolled in daycare?" yielded the following references:
https://jamanetwork.com/journals/jamapediatrics/fullarticle/191522
https://pubmed.ncbi.nlm.nih.gov/2007922/
https://pubmed.ncbi.nlm.nih.gov/11296076/
https://pmc.ncbi.nlm.nih.gov/articles/PMC5588939/
a CNN article that pointed to https://pubmed.ncbi.nlm.nih.gov/21135342/
and an Emily Oster blog post which links to some other relevant studies.
I haven't gone through any of the above links in detail just now, but the general message one gets from the abstracts seems to be an increase in frequency for years 1-2, then back to baseline. Some suggest some protective effect in early elementary school years (the first link, which is the Tuscon study OP mentioned; the Côté paper that the CNN article pointed to; and apparently the Hullegie et al. 2016 study OP mentioned, which wasn't among those that Claude dug up).
The Søegaard et al. study highlighted by the OP has an interesting couple of figures 1 and 2, for boys and girls respectively. These are differences in infection rate per year for four groups, compared to children never in childcare. Since this is Denmark I'm guessing the "instition enrollment at 3 yrs" is kids who started børnehave (preschool) at age 3.
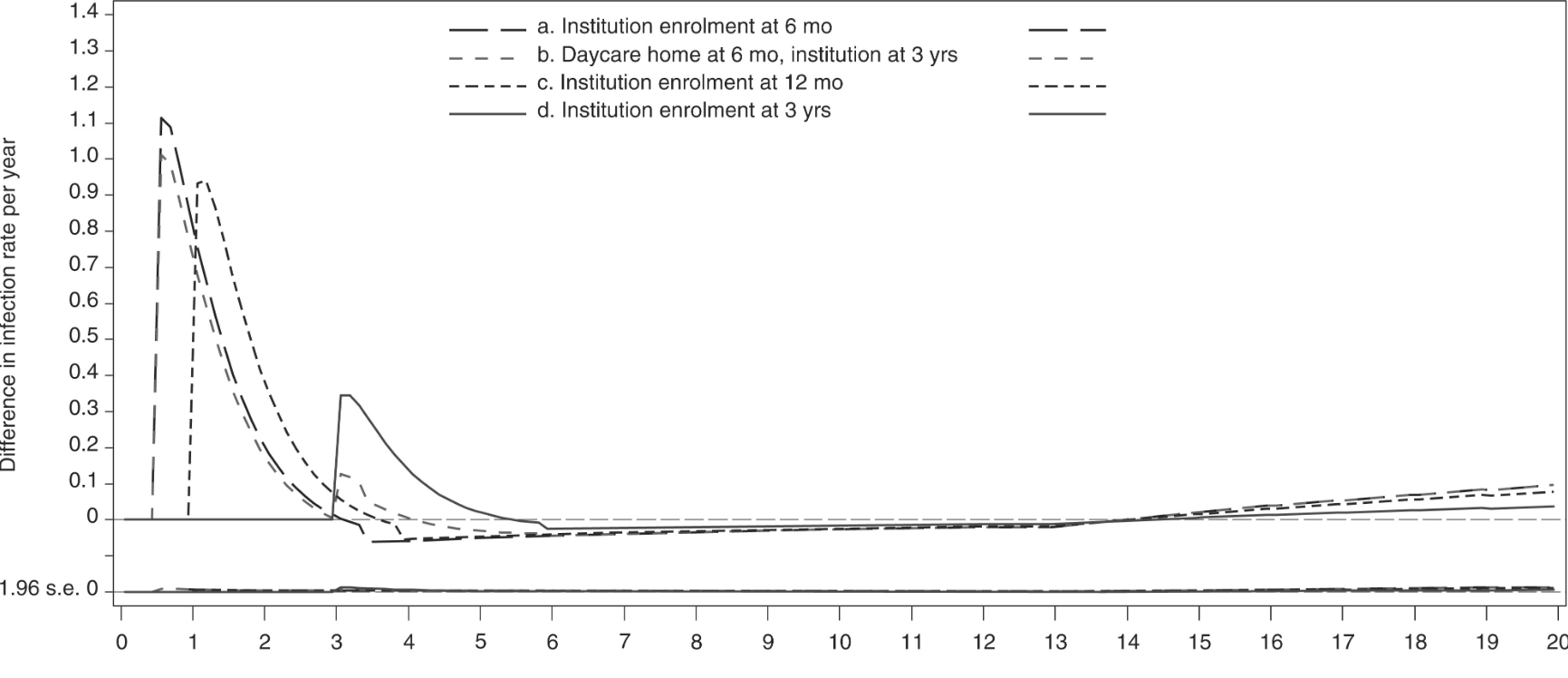
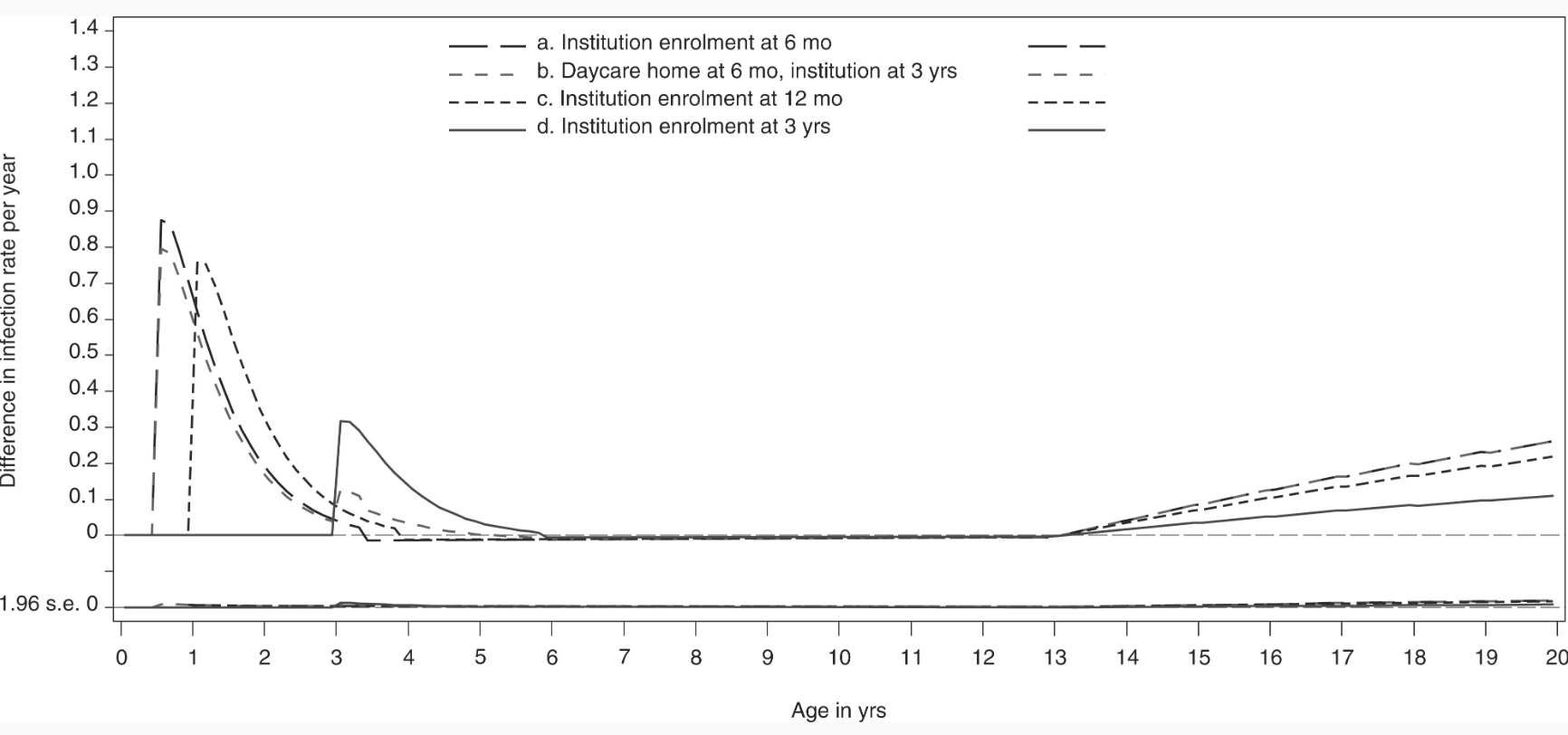
This does look like it shows some amount of immunity happening: otherwise, we'd presumably expect to see group (b) having a spike as high as group (d) at age 3 yrs. Though importantly it isn't enough to compensate if what you care about is total number of illnesses avoided. [1]
Also, although the spikes look quite dramatic, the y-axis shows that the difference in infection rate per year is approximately 1 for the highest spike in each graph. Similarly, the abstract notes that children enrolled in childcare before age 12 months had experienced 0.5 - 0.7 more infections than peers enrolled at 3 years, cumulatively, by the time they got to age 6 years. To be sure, that certainly corresponds to more than one actual infection, since "infection" in this paper means an infection serious enough to result in an antimicrobial (usu. an antibiotic) being prescribed, but is not an enormous effect.
Regarding the beliefs and confidences listed in the post:
- (Quite confident) The most common illnesses (colds and flu) don’t build immunity in general (in kids or adults) because they mutate every year
- (Quite confident) The same illness has a greater risk of complications in babies vs. older children and adults
- (Moderately confident) The same illness has a greater duration in babies vs. older children and adults
- (Moderately confident) Illness during early development is probably more harmful than illness during adulthood
- (Weak guess) Daycare environments are more conducive to disease spread than schools for older kids and the number of possible illnesses is very high; there isn’t just a limited number of things you catch once
For #1, I think my level of agreement depends on exactly what is meant by "immunity in general". Claude's answer to "Does catching viruses improve your immune system long term?" can be summed up as (in Claude's words): "Surviving one virus generally makes you better at fighting that specific virus (and sometimes closely related ones). It doesn't broadly upgrade your immune system's ability to handle unrelated threats." This matches my previous understanding.
However, due to the caveat about "and sometimes closely related ones", I think this is consistent with the claims of lower rates of illness in early school ages reported by Tuscon / Côté / Hullegie, and the difference between lines (b) and (d) at age 3 in the Søegaard graphs. My understanding is that even though viruses mutate all the time, many remain "closely related" to the versions they mutated from, and this confers some protection from infection and/or severity. For example, if I remember correctly from back when I was doing a lot of reading on COVID, the consensus was that after repeated and significant mutations, protection given by a vaccination based on an older strain gave limited or no protection from infection (no longer recognized by B cells), but still gave significant protection from severe infection, since the epitopes recognized by T cells remained consistent. Something like this goes for flu viruses also (look up "heterosubtypic immunity") and I believe common cold coronaviruses too.
That said, I am a bit baffled by the lack of any dip at all for the nursery groups below the baseline at age 6 (when Danish compulsory education starts) in the Søegaard graphs.
#2 seems true for most illnesses, and seems likely to be an underappreciated consideration. My understanding is that children under 1 year old are particularly vulnerable.
I hadn't really thought about #3-4 and haven't taken the time to dig up relevant literature to see if I agree, but they seem plausible: if true, then they should also inform one's calculus.
Less certain about #5 (seems likely to be technically true, but not sure it moves me very much one way or another given my beliefs on the others and the data from the studies above).
An additional consideration is that there is some evidence that catching COVID can have long-term negative effects on the immune system, although COVID is also weird in that children fare better than adults with it overall.
So, considerations pointing in both directions. I will say that in our own case I am happy we made the decision to start our son in daycare shortly after his first birthday, particularly given that our alternative was one parent quitting a fulfilling job to stay at home (IIRC there were no available full-time nannies or au pairs in our area, or at least none at a cost we felt we could remotely afford). This would have been a financial hit that probably would have required us to take on substantial debt, and also would have been incredibly challenging. Additionally, the level of different experiences and socialization our son gets on a daily basis is well beyond what we could realistically provide on our own, and he loves it.
So for our family, daycare has been worth the illnesses. But of course we would be biased to prefer the decision we actually made, and might feel differently if we'd had a worse experience. And I won't pretend that the first year of it was easy: due in part to her asthma, my wife got pneumonia twice. (We've used this as an excuse to get the daycare to allow us to wait to pick him up outdoors, rather than in the cramped coatroom in which every other child and parent breathes in from 5.30-6pm).
- ^
Regarding the reference group and the weird increase after age 14, the authors write:
We observed slight increases in the infection rates and cumulative number of infections at ages 14–19 years among children enrolled in childcare during the first 3 years of life compared with peers in homecare, which were most pronounced among girls. However, these increases were proportional between the different enrolment types (ages at enrolment and types of facilities) and thus appeared to be a phenomenon related to the reference group comprising a small number of children who remained in homecare during the first 6 years of life (0.7% of the total cohort). Thus, although we adjusted for maternal education and income, maternal smoking, maternal age at delivery, ethnicity and child’s diagnoses of chronic diseases among other factors, we cannot rule out that the observed increasing rates and cumulative number of infections in adolescence associated with childcare attendance were due to residual socioeconomic confounding.
Similarly, the abstract notes that children enrolled in childcare before age 12 months had experienced 0.5 - 0.7 more infections than peers enrolled at 3 years, cumulatively, by the time they got to age 6 years. To be sure, that certainly corresponds to more than one actual infection, since "infection" in this paper means an infection serious enough to result in an antimicrobial (usu. an antibiotic) being prescribed, but is not an enormous effect.
I wonder why you conclude this 'is not an enormous effect'. Maybe it's differences in antibiotic usage between countries, and you're from a country where it's more common? Because for me it seems like a really big deal to have like 1 in 2 kids needing an extra treatment of antibiotics before they're 6 years old.
I think Denmark has lower general usage of antibiotics than the United States for example (I think 70% as much, if I just divide the Defined Daily Dose by the population.) And I guess the gap is bigger for smaller issues, as I expect more critical situations to always result in antibiotics usage whether you're in the US or Denmark.
I'm not an expert in this field, nor did I check the statistics carefully, this is mainly based on the feeling I get when foreigners come to the Netherlands (60% DDD per person antibiotics usage compared to Denmark) and complain that they don't get antibiotics when they get the sniffles.
https://www.pnas.org/doi/10.1073/pnas.2411919121#supplementary-materials
"Constantly being sick as a baby/toddler or not" does seem like the sort of thing that could make a few IQ points worth of difference. Some things I found with Claude on a quick initial search:
- This study found that a single infection resulting in hospitalization before the age of 19 was associated with an IQ 1.76 points lower at age 19, which shrunk to 1.13 points after adjusting for some confounders. They also found that the effects of these severe infections stacked, moreso if subsequent infections were of different types.
- This one found that a single infection resulting in hospitalization before the age of 13 was associated with an IQ 1 point lower at age 18; 1.61 points lower if the infection was before the age of 1. The effects shrunk a lot after the age of 1: -0.7 points for ages 2-4, -0.26 points for ages 5-9, -0.12 points for ages 10-13. These effect sizes come from a model controlled for some confounders.
- Another study found that having had any acute respiratory illness (ARI) before age 1 was associated with a 3 point lower Bayley score at age 1, but any ARI before age 2 was not significantly associated with score at age 2. (The Bayley is basically an IQ test for babies. If done at age 2 it probably correlates with adult IQ at something like r=0.3; even less if done at age 1.)
- A study with a negative result: infections recorded between birth and age 5 were not significantly associated with IQ at age 11.
(Note: these could have been selected for positive results, either through publication bias or Claude searching.)
I do not have children, but I do have a biology PhD, so that's definitely equivalent. Re: Søegaard et al. 2023
Antimicrobials redeemed were antibacterials (90.5%), anthelmintics (7.8%), and antifungals, antimycobacterials, antivirals and antiprotozoals (combined 1.7%).
[...]
we used prescriptions for antimicrobials as a proxy for infections, but our study does not inform about the potential impact of childcare enrolment on milder infections not requiring treatment or on more severe infections leading to hospitalization. Also, the majority of infections in early childhood are viral rather than bacterial.
they then claim
However, we presume that variations in viral infection rates associated with age at childcare enrolment would resemble those observed for primarily bacterial infection rates in our study. This is supported by the observation that seasonality of viral respiratory infections correlates closely with that of antibiotics use in Danish children.
but skimming through the references "closely correlates" doesn't seem well supported, other than that both occur more in the winter. Also, the references only track hospitalized viral pneumonia (probably because they don't have the data for mild infections).
We observed slight increases in the infection rates and cumulative number of infections at ages 14–19 years among children enrolled in childcare during the first 3 years of life compared with peers in homecare, which were most pronounced among girls. [...] Thus, although we adjusted for [a lot of factors], we cannot rule out that the observed increasing rates and cumulative number of infections in adolescence associated with childcare attendance were due to residual socioeconomic confounding.
I'm not sure I'd call the increase "slight"; but there definitely seems to be some issue with the control group.
When enrolling in daycare, there's a spike of infections, then a decay afterwards, which you would expect if you started developing resistance to infections. So they are acquiring immunity, that is clear; the question is whether this acquired immunity is (on net) beneficial.
--
Re: claims
(Quite confident) The most common illnesses (colds and flu) don’t build immunity in general (in kids or adults) because they mutate every year
I'd walk back the confidence on this; just because they mutate every year doesn't mean it's not building immunity. Infection generates many different antibodies, and if any of those antibodies bind (even if not perfectly), then it provides immunity. It may not be perfect immunity, but may weaken severity.
And you don't notice how many times your has fought off an attempted infection, you only notice when it fails.
(Quite confident) The same illness has a greater risk of complications in babies vs. older children and adults
(Moderately confident) The same illness has a greater duration in babies vs. older children and adults
(Moderately confident) Illness during early development is probably more harmful than illness during adulthood
Yes, I'd say that's generally true. Though there might be a developmental window for immunity (see: allergies) and sometimes the immune response in adults is more dangerous (see: chickenpox).
(Weak guess) Daycare environments are more conducive to disease spread than schools for older kids and the number of possible illnesses is very high; there isn’t just a limited number of things you catch once
Daycare environments are more conducive to disease spread probably due to a lot more touching and less sanitation. I think the number of possible illnesses is very high, but it's a mix of things you can catch once and things that mutate that build (partial) immunity (see point one).
--
Immunologically speaking I don't think we understand development enough to give strong recommendations. Exposure is definitely helpful in building an adaptive immune response, but what age is best is an open question. Vaccines definitely have less side effects than an infection, but (some) vaccines might produce antibodies biased towards one protein instead of the whole virus, which may not provide as broad immunity.
In my opinion Chesterton's Fence remains in place (especially if it's cost-effective for other reasons), but more research is required.
A lot of your comment makes sense, but it feels like a stretch to invoke Chesterton's Fence here? Daycare is a relatively recent invention that we do know the purpose of.
I agree invoking Chesterton's Fence may not be exactly fit for purpose.
But since we know it's purpose (increased workforce participation), you can choose to remove it if it makes sense for your circumstances (able to leave the workforce to take care of your child). Any positive/negative -ternalities of children in daycare (illness, immunity) are not strongly supported, but we do have about a hundred years of history saying that it's probably not (measurably) harmful.
But also, as with most things, too many changes are happening at once. Is daycare closer to pre-industrial childrearing with larger families and village-raising, compared to modern single-family single-child care? Daycare probably mixes more germs just through larger geographic distance (smaller daycares with more continuous groups of children might work better, but also probably more expensive).
also, do we want preindustrial childcare? child mortality wasn't great back then, and it is unclear how much of that can be linked to childrearing practices.
no clear answers, only more questions
Exposure is definitely helpful in building an adaptive immune response, but what age is best is an open question.
We have to distinguish between the biological fact of establishing an adaptive immune response and the practical implication that chronic childhood infections are not worth avoiding or are net beneficial. We can't assume that the marginal expected effect of an infection at any age is beneficial to health.
Sure, you can live the rest of your life in a perfectly sterile environment, but then other costs are at play in sustaining that.
It's an interplay between severity of disease at age, chronic effects, and cost of avoidance.
As you know, there are immunocompromised children who are forced to live in perfectly sterile environments. That is clearly not what I am talking about.
A scientist’s job in public communications is to help separate the facts we know from the uncertainties, and the positive questions from the normative.
Strawman statements like “sure, you can life the rest of your life in a perfectly sterile environment” are the opposite of that. They encourage audiences to collapse those vital distinctions and introduces unnecessary volatility and distraction into the discussion.
I don't think your framing is helpful.
I framed the question as "is it better to get sick earlier or later" and you said "actually, it's better not to get sick". Yes, that is technically correct, but is also not engaging with the question, and also not at all practical.
EDIT: perhaps I read your comment incorrectly, but this is how I interpreted it.
I think from context and from the article I'm commenting on that it was obvious I was talking about relatively mild childhood infections with few long-term effects (that we know of). I was not talking about polio, or HIV, or Ebola. I thought it was clear, but perhaps it was not.
There is a separate question on whether what we think are benign childhood infections have long-term negative consequences that we consider normal or normative. That may be possible, but given the wide prevalence of these pathogens the question again becomes whether you are infected earlier or later, or if you can spend your life in a sterile bubble.
When enrolling in daycare, there's a spike of infections, then a decay afterwards, which you would expect if you started developing resistance to infections. So they are acquiring immunity, that is clear; the question is whether this acquired immunity is (on net) beneficial.
It's also about how long lasting the immunity is. If the immunity lasts 1-2 years, you aren't gaining that much.
If the immunity is short-lived, we would not expect the decay to persist (which is does to age 13 independent of age of entry into daycare, Figure 1 and 2). It takes about 3 years for the number of infections to decay back to baseline (no more infections than children who do not go to daycare); if immunity was short-lived, we could expect a spike as one is exposed to new pathogens, then settling to a low baseline level of infection as immunity wanes and reinfection occurs, but we don't see a higher baseline (or if the baseline is higher, it is hard to see).
One could argue that the decrease in infections is due to age-dependent immune system development instead of an adaptive response, but then the different age-of-enrollment decay curves should overlap, which they do not. Later enrollment does lower the magnitude of the initial spike, which suggests that there might be an effect, but the non-overlapping decay curves implies that adaptive immunity is playing a role.
I'll definitely run your article by my wife (Biology PhD), who's better situated than I am to comment on the science than I am.
We have two kids and use the university's daycare. It certainly feels like it's the case that we get sick much more often as a result of daycare usage. So far, we've decided to eat this cost for a number of reasons (many of which will not apply broadly):
- Our daycare is extraordinarily convenient. We hold hands and cross the street. There it is.
- We love the teachers, the free play, the outdoor space, and the overall teaching philosophy.
- Our daycare is slightly subsidized relative to other Palo Alto daycares.
- Vetting a daycare felt easier than vetting nannies (more parents to talk to; generally a longer history of care). Also, more seems to ride on the choice of nanny in the sense that one person will have a lot more influence on the kids than a team of teachers (though arguably this unlocks more benefits if you are able to find an incredible nanny).
- We have learned to cope with illness. Nothing will take away all the terribleness, but we're pretty proactive with ibuprofen, Tylenol, and anti-nausea medication. We've also learned that if we do saline rinses as soon as either kid has a stuffy nose, it seems to greatly reduce the number of ear infections they have.
- I have a flexible job that lets me work from home and request back-up care on short notice. I'm mostly able to absorb the sick days in this way.
My wife would have a more nuanced view of the studies you cite. I do have this general impression that lots of parents are over-stressed as a feature of our mega-society, high-information exchange modern environment. Like, today, as parents, we are confronted with the kind of stories and data you only get if you are part of million-member+ society. It's easy to feel haunted by all kinds of terrible stories and outcomes where, in reality, many of them are on par with other risk I've internalized (e.g., car accident risk on the way to the grocery store) (which is not to say we shouldn't take car accident risks seriously).
This would seem to differ from our ancestral environment, where the data and folk traditions from maybe ~10,000 persons pointed more directly to high risk and high impact harms. "Do not eat that specific mushroom" or "Warn the kids about the river and supervise trips near the river more closely."
I think our brains have trouble processing rare but high impact risks communicated out of our mega-societies, in part, because there are many, many, many more we have to track now. Don't get me wrong—I am grateful that our mega-societies are helping us understand and mitigate child suffering. But I also think our poor ability to process all these risks may itself lead to actions which carry future risks on par with the risks we were supposed to be mitigating. It does not seem implausible to me that high parental stress or overbearing supervision may have serious downstream consequences on child welfare.
All of this is to say that, assuming daycare has significant convenience/happiness benefits and the studies show marginal risks (perhaps on par with other risks you have deemed appropriate), it can be okay to say, "I know we will be sick more, but this is still good for us."
I hope I won't be cooked here too much for my phrase "deem appropriate." I'm not saying that in the sense that I've become indifferent to certain risks and harms (or worse, embraced them in the "sour grapes" way). It's just to say that certain risks seem very difficult to avoid (e.g., transporting my child) and worrying about them past a certain point would seem detrimental to my mental health and my overall ability to function and flourish in this risky world of ours.
I'm not going to cite a bunch of papers because I'm choosing between (1) writing something fast or (2) not at all, but my current posteriors on the causes of adult intelligence load non-trivially on genetics, but to the degree that parents control how smart their kid grows up to be, almost all of those effects for "the kinds of parents who could adopt kids with that level of parenting" (and aren't alcoholics, or effectively illiterate, or moderately neglectful, or giving them apple juice instead of milk every day...) the influence seem to route through raw brain health due to good nutrition and low disease burden, especially under the age of 6?
Basically, my central mechanistic posterior is that the brain is really GROWING and establishing itself when you're 1 and 2 and 3 and 4.
If your body doesn't get high protein levels or is wasting energy fighting off diseases, then the brain establishes itself less well, in ways that will echo through all future decades.
This is why (according to the posteriors in my brain, and no particular studies I'm going to look up) schooling prior to kindergarten hurts adult IQ in children whose parents are rich and could care for them very well.
And it is why schooling somewhat helps in children whose parents don't read to them, don't have middle class culture to transmit to them, and who might not even be feeding them adequately...
Exposure to "decent care from civilized people" AND DISEASES FROM PEERS can be a real net help for a 36 month old child who gets decent orderly care from nowhere other than government funded minding by non-family (even if the 36 month old will be near a bunch of other kids, and get sick from that, and get very slight brain damage from the sickness).
Before I had a baby I was pretty agnostic about the idea of daycare. I could imagine various pros and cons but I didn’t have a strong overall opinion. Then I started mentioning the idea to various people. Every parent I spoke to brought up a consideration I hadn’t thought about before—the illnesses.
Reading this, I was surprised that people were tracking the single biggest mechanistically controllable variable because normally people aren't tracking evidence or reason or their goals or what the best way to get what they want is!
Invariably every single parent who had tried to send their babies or toddlers to daycare, or who had babies in daycare right now, told me that they were ill more often than not.
One mother strongly advised me never to send my baby to daycare. She regretted sending her (normal and healthy) first son to daycare when he was one—he ended up hospitalized with severe pneumonia after a few months of constant illnesses and infections. She told me that after that she didn’t send her other kids to daycare and they had much healthier childhoods.
This was a second surprise, but it ameliorated the first surprise. Initially I thought that people had actually read the papers I had, and come to the same conclusions, but here it sounds like they are just having their noses rubbed into the mechanism of disease burden over and over and over and telling stories about it...
...which is a very valid way to make local sense of your local world! <3
Basically, my posteriors here are that the effect sizes (exposure to an diseases vs conscientious adults) go in different directions and ~~balance out for kids with bad parents (and they can actually be net positive for very bad parents).
Whereas if the parents are good, the adult IQ is higher if they skip school until they are five or six years old and their brain is sort of done with most of the core biological developmental steps (they're passing mirror tests, passing sally anne tests, seriating, and so on).
The effects on raw brain health and later adult IQ consequences aren't enormous either way...
But since IQ has broad consequences across many areas of life... maybe optimize for that?
And in that case the rough prescription I would offer is that good parents should keep the kids home if they can (or at least choose the daycare that keeps statistics on child diseases, isolates sick kids, brags about the low disease burden, and generally has decent "public health" practices) and bad parents should sent them to state subsidized daycare for better food and some structure in their life even if the diseases DO cause (very mild) brain damage.
This does remind me of Gunnar creating a linkpost for Childcare : what the science says. According to it daycare seem to raise cortisol levels in the children.
That must have been the one I read and which informed my decision to minimise daycare hours for my son.
(Quite confident) The most common illnesses (colds and flu) don’t build immunity in general (in kids or adults) because they mutate every year
My impression was that you have partial immunity to viruses that are mutated versions of ones you've already been exposed to.
See for example: https://en.wikipedia.org/wiki/Original_antigenic_sin
Plus there's also cytomegalovirus (CMV) which spreads a lot at daycares and causes lifelong infections with negative effects years later. https://denovo.substack.com/p/cytomegalovirus-the-worst-herpesvirus
We moved to an outdoor-only preschool and it seems to have helped. (Two step, the sickness was too much and we pulled from daycare, then our kid was clearly missing socializing so had to find a compromise and outdoor looked good)
I read a review about daycare which came to the conclusion that daycare before the age of two had clearly negative effects on the kids, between two and three it was mixed, and after the age of three it was positive (no daycare wasn't an option for us but this was the reason we reduced hours as much as possible). The reason given was that it is stressful for little kids to be separated from their mom. But now I wonder whether infections don't play a bigger role than that. Luckily my kids are pretty robust in that regard.
(Quite confident) The most common illnesses (colds and flu) don’t build immunity in general (in kids or adults) because they mutate every year
Not my area, but it seems like the difference between "this year's variant and last year's" is going to be much, much smaller than the difference between "never exposed to any cold/flu before".
So naively it seems possible that the first several colds do train the immune system quite a bit to handle colds in general, even if subsequent ones are then moving around to different points on the fitness landscape.
Yes. There are many different "cold" viruses, and adults have some degree of immunity against most of them, while children are getting many for the first time in their life. That's very different from the flu, which doesn't have many concurrent versions but is evolving more rapidly. (Not sure where covid falls here.)
There's always been jokes about how often day care kids get sick, but I feel like it didn't used to be more sick days than healthy. I did some AI searches but they didn't turn up good time series on this.
If it has indeed changed for the worse, one possible cause to investigate is whether kids come to a particular daycare from a wider area, and so sample diseases from a larger population.
I believe you're roughly correct on all points. I have a 2yo who has been sick more than not, and we the parents too.
Ultimately it's a question of means, at least for us. If we could afford not to send our kid to daycare, we probably would do just that.
(Layman disclaimer) The human immune system has not evolved in dense population. Bats are built differently. Evidence for immunity building looks to me like the studies mostly compare nature kids with indoor dwellers. Outdoor play has way more distance, fresh air and little shared surface.
Despite all this, many parents who have the option not to (i.e. they can afford in-home care with a nanny or for one parent to stay home) still choose to send their babies and toddlers to daycare. How come? Surely most well-off adults wouldn’t agree to be ill nonstop in exchange for the monetary savings daycare provides?
My experience of day care (admittedly, a small one with < 10 children), is that the incidence and severity of illness is very low relative to how it is described in this article. Last year, I had to keep one or the other child home from day care on no more than thirty occasions. In basically every one of these occasions, the child had a runny nose and maybe a slight fever. Every instance of more severe illness that we suffered in the same time span (no more than five occasions) occurred on vacation and was unrelated to daycare. Maybe we are incredibly fortunate. I believe the biggest negative effect on my children from these bouts of illness will be that they missed out on being at daycare and watched a lot of TV because I usually had to work on those days. I do not think the illness itself will have any quantifiable effect on their lifetime earnings.
We could have further reduced this disease burden by having one of us quit our job to parent at home. This would have cost us at the very least $50,000 in foregone income net daycare costs, and probably a lot more in terms of career development. We could have hired a nanny for an additional $25,000 a year.
In my opinion, the benefit of reduced illness would probably not justify the expense. We are wealthy enough to afford the nanny option, but not so wealthy as to find this a good use of those funds.
Just to provide counter-data: we started the kid off at 2y3m in kindergarten with about 13 kids total. He's been sick maybe 1 or 2 times in the past 6 months; similar to the rate he'd usually get sick, but we do take him to playgrounds and other places with other kids a lot anyway so maybe the difference is not that big. I'd assume that the kindergarten having air filters and very few kids (13 is not the size of his group, it's the whole institution, and all the kids are together), makes this a much more reasonable trade-off between socializing and illness.
Is there any commentary on breastfeeding bias in the studies? It is my understanding that breastfeeding provides significant immune support to babies. I would guess that babies attending daycare are biased towards less breastfeeding.
Before I had a baby I was pretty agnostic about the idea of daycare. I could imagine various pros and cons but I didn’t have a strong overall opinion. Then I started mentioning the idea to various people. Every parent I spoke to brought up a consideration I hadn’t thought about before—the illnesses.
A number of parents, including family members, told me they had sent their baby to daycare only for them to become constantly ill, sometimes severely, until they decided to take them out. This worried me so I asked around some more. Invariably every single parent who had tried to send their babies or toddlers to daycare, or who had babies in daycare right now, told me that they were ill more often than not.
One mother strongly advised me never to send my baby to daycare. She regretted sending her (normal and healthy) first son to daycare when he was one—he ended up hospitalized with severe pneumonia after a few months of constant illnesses and infections. She told me that after that she didn’t send her other kids to daycare and they had much healthier childhoods.
I also started paying more attention to the kids I saw playing outside with their daycare group and noticing that every one had a sniffly nose.
I asked on a mothers group chat about people’s experiences with daycare. Again, the same. Some quotes:
“They do get sick a lot. I started my son at 2.5 and feel he always has something.”
“The limit does not exist.”
“brought home every plague (in first 6mo, Covid, HFM, slapcheek, RSV)”
“They usually say 8-12 illnesses per year. My girls were sick every 2-3 weeks in their first year of daycare”
“My daughter started daycare at 6 months and got sick a ton the first year”
Despite all this, many parents who have the option not to (i.e. they can afford in-home care with a nanny or for one parent to stay home) still choose to send their babies and toddlers to daycare. How come? Surely most well-off adults wouldn’t agree to be ill nonstop in exchange for the monetary savings daycare provides?
Asking around, it seemed like the most common reason given was that parents believed daycare illnesses “built immunity”; that if their babies and toddlers got sick at daycare they’d get less sick later in childhood and so overall it would net out the same. Unfortunately few could point me to any evidence for this but nevertheless passionately defended the view.
The claim that daycare illnesses simply offset childhood and adult illness immediately seemed suspect to me for a number of reasons:
I xeeted about this:
A number of people sent me this link, an alleged “study” from UCL showing that “frequent infections in nursery help toddlers build up immune systems”, authored (of course) by a group of parents who all send their kids to nursery (what the British call daycare).
The link I was sent was actually a UCL press release summarizing a narrative review paper and not a study itself. Narrative reviews are susceptible to selection bias because, unlike systematic reviews or meta-analyses, there’s no pre-registered search protocol or PRISMA-style methodology requiring them to account for all relevant evidence. But I decided to look into the narrative review more, to assess its validity fairly. I got access to the full publication.
Unlike the press release, which ignores these considerations entirely, it does engage with severity and age-related vulnerability, conceding that younger toddlers and babies suffer more from the same illnesses. A section on immunology provides a detailed account of why infants under two are more vulnerable—their immune systems are much less effective at fighting the same infections for a plethora of well-understood reasons. The review also cites a large Danish registry study (Kamper-Jørgensen et al) that reports a 69% higher incidence of hospitalization for acute respiratory infections in under-1s in daycare.
However, these severity findings are integrated into the review’s conclusions and framing in an incredibly biased way. The introduction describes severe outcomes as occurring “in rare cases,” and the conclusions focus on normalizing the burden and advocating for employer understanding. After establishing the immunological basis for why the same infection is more dangerous in a 6-month-old than a 3-year-old, it doesn’t then ask the hard follow-up question: given this, is the pattern of starting daycare at 6–12 months optimal from a child health perspective? Instead, the review frames this timing as a societal given. The Hand Foot and Mouth Disease section is a good example of the review’s handling: it reports that daycare attendance was associated with more severe cases but then immediately offers mitigating interpretation with no evidence—that prolonged hospital stays might reflect parental work constraints rather than genuine severity.
Though the review considers severity, it ignores duration. Their primary metric throughout is episode count. Also, despite discussing a wide variety of pathogens, it doesn’t address which of these infections carry the highest complication rates in infants and toddlers specifically.
Finally, the crucial “Illness now or illness later?” is the paper’s weakest portion. It rests on two primary sources for the compensatory immunity claim:
These are reasonable small studies, but the paper does not cite or engage with the Søegaard et al. 2023 study (International Journal of Epidemiology)—a register-based cohort of over 1 million Danish children followed to age 20, which directly tested and rejected the compensatory immunity hypothesis. Quoting from the study:
This is arguably the single most relevant study for the paper’s central “illness now or illness later” question, and it’s three orders of magnitude larger than either study the authors cite. Its absence is hard to explain—it was published in a top epidemiology journal in late 2022 (available online November 2022), well before the review was written.
Accordingly, they hedge their conclusions carefully—“attendance at formal childcare may tip the balance in favor of infection now rather than later”, but their press release ignores any nuance, referring to daycare as an “immune boot camp”.
So overall, the compensatory immunity claim seems very weak and my prior that daycare illness is straight-up bad remains. Parents are citing biased reviews from motivated researchers. We are only beginning to understand the deleterious effects of increased viral load in infants.
I predict that in the future we’ll learn more about the side-effects of increased viral load on intelligence, wellbeing, fatigue etc. The “just the sniffles” mentality is a harmful attitude toward infections that promotes the dismissal of phenomena that substantially impact child and adult wellbeing.