Epistemic status: I am not a doctor. This is based on a combination of the most rigorous medical lit searches I could do over several hours, and individual reports that may or may not be based on anything. Wherever possible I’ve provided links to my sources so you can form your own opinions.
This is based on my best knowledge right now. I could be missing things, or new information could come to light, in which case I will update this as quickly as possible (and appreciate holes being pointed out).
Uncontroversial
That's an excellent question, but the more I research it the less confident I am in any particular answer. My eventual conclusions will be going up at this question, although right now I think the answer is going to be "feel sick? then maybe."
This depends in part on how functional your medical system is. If you’re in a place where you can get a drive by test and your doctor will order you experimental drugs over the phone, maybe do that. If you’re in the US, I don’t expect calling a PCP to do much even if you have one, which many people don’t. So your choice is “When do I go to the hospital?” keeping in mind that the hospital is well over capacity and that if you don’t have COVID going in, you’re likely to catch it there.
So I personally wouldn’t go to a hospital unless I clearly needed something I couldn’t get at home, which basically means oxygen or whatever they do when your fever is dangerously high for too long, which means “when I struggle to breathe” or “when my temperature is over Nº and antipyretics won’t bring it down”.
In a few places above I advise you to call your primary care physician, knowing full well many people don’t have one and that there’s not a lot they can do for COVID. That’s more ass-covering and future-proofing than anything; I’d feel really bad if it turned out they could do something and you missed out because I told you not to.
> It is probably too late though.
That might be technically true but I think it's misleading - I'm not clear on how common it was in China for one member of a household to get sick and others to stay well, but from anecdotal reports in the US I think it's fairly common for one person to get it and not spread it to e.g. their spouse and children.
So I'd think if one member of a household has symptoms, it's well worth quarantining within the household instead of assuming it's not worth trying to limit spread.
It's also important not to think of infection as binary, all-or-nothing: minimizing your cohabitants' inoculum may reduce the likelihood they get a severe case (I don't really know, I would just suggest that it's a possibility worth checking.)
Do you have a runny nose? Probably not COVID-19
I'm concerned about this one as advice. I think it's fine to say it's a likelihood ratio of 20x against, but the in presence of severe fever, cough, and difficulty breathing, I think a person should still place non-negligible probability on it being COVID-19 notwithstanding having had a runny nose at some point. I'm worried people about hearing the "runny nose != COVID" updating too hard that they don't have it. 1 in 20 people isn't that rare.
I think it's more reasonable to say that if you don't have fev
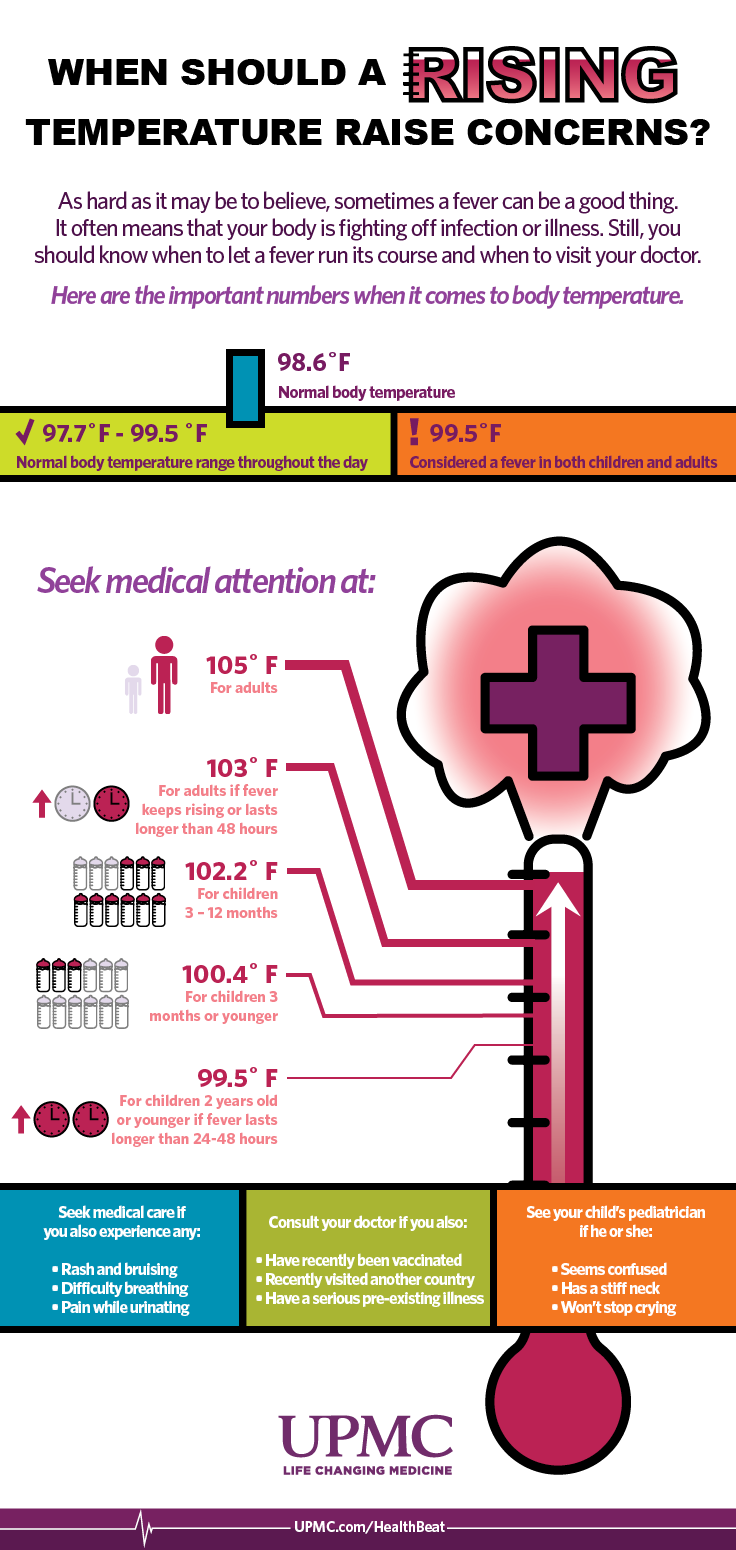
This image looks like a good guide of when to seek medical attention for a fever:
As I reach for the Ibuprofen and hesitate:
France is recommending against NSAIDs and against ibuprofen in particular. I will be very surprised if that ends up being born out (and WHO agrees with me)
Which part of the WHO status makes you think they don't think it will be born out? It says they're recommending what France says for now even though they don't currently have evidence that it's a problem.
I would advise against taking zinc lozenges. Zinc may at best shorten the duration of a cold caused by rhinovirae by 1 day. But the side effect may be a permanent loss of smell. AFAIK there are no studies showing it to have any measure-able effect on COVID. Chloroquine does not seem to be useful against COVID whatsoever. Initial studies of it were flawed and had a too small sample size. Taking Chloroquine probably does more harm than good.
Take chloroquine or hydroxychloroquine along with zinc ASAP (so you can avoid being hospitalized). ETA: Preferably after talking to your doctor about it. See references below for more details. If you didn't buy chloroquine/hydroxychloroquine ahead of time, beg your doctor for a prescription, or call doctors around you until you find someone willing to give you a prescription (because unlike China and South Korea, it doesn't seem to be part of the standard treatment for COVID-19 in the US).
ETA: Some relevant information from the CDC:
Based upon limited in-vitro and anecdotal data, chloroquine or hydroxychloroquine are currently recommended for treatment of hospitalized COVID-19 patients in several countries. Both chloroquine and hydroxychloroquine have known safety profiles with the main concerns being cardiotoxicity (prolonged QT syndrome) with prolonged use in patients with hepatic or renal dysfunction and immunosuppression but have been reportedly well-tolerated in COVID-19 patients.
[...] Hydroxychloroquine and azithromycin are associated with QT prolongation and caution is advised when considering these drugs in patients with chronic medical conditions (e.g. renal failure, hepatic disease) or who are receiving medications that might interact to cause arrythmias.
Quoting Rob Wiblin:
"DO NOT TAKE IT OUTSIDE MEDICAL SUPERVISION: "Chloroquine is very dangerous in overdose.""
https://www.facebook.com/photo.php?fbid=886113990345&set=a.509700885225&type=3&theater
Just because something is dangerous in overdose doesn't mean that medical supervision is needed: for example acetaminophen, or even water. The relevant thing is that the therapeutic dose is close to the lethal dose for chloroquine, and chloroquine dosing is complicated.
Hydroxychloroquine is 40% less toxic while still being effective, according to this article: https://www.nature.com/articles/s41421-020-0156-0
Medical supervision may not be available if current trends continue, so we must carefully weigh the options available to us.
This sounds like a prime opportunity for people with medical expertise to write guidelines on how to use it for civilians.
Here's a negative study about hydroxychloroquine that just came out: http://www.zjujournals.com/med/EN/10.3785/j.issn.1008-9292.2020.03.03 (archive link because the website seems to be down)
I think this is unsafe advice, specifically using chloroquine and hydroxychloroquine without medical supervision.
These are not benign drugs (chloroquine being worse) and you are advising people use it while unwell with an emerging and poorly understood disease that could potentially alter its safety and pharmacokinetic/dynamic profile, and without any consideration for potential other health issues people have or medications people are taking (eg many antidepressants and anyone with diabetes).
If you have chloroquine/hydroxychloroquine, you should go see yo
Of the initial 26 in the treated group:
no one left the control group.
"We left out four patients who got definitively worse" seems like a big flaw in the analysis.
It's still available on the Internet Archive: https://web.archive.org/web/20200319023745/https://docs.google.com/document/d/e/2PACX-1vTi-g18ftNZUMRAj2SwRPodtscFio7bJ7GdNgbJAGbdfF67WuRJB3ZsidgpidB2eocFHAVjIL-7deJ7/pub
You can buy hydroxychloroquine here still (as of March 20th): https://fixhiv.com/shop/coronavirus-drugs/hcqs-400-hydroxychloroquine-400-mg/ which imports it from India. This site also lets you easily buy a prescription for it, FWIW.
Check for G6PD deficiency before taking chloroquine (can be done through the 23-and-me interface) as it can cause haemolysis. Apparently not an issue with hydroxychloroquine: https://www.ncbi.nlm.nih.gov/pubmed/28556555
I read a lot of recommendations for electrolytes but found all of the explanations kind of vague, so I did 2 hours of digging (plus more research from Eli Tyre). This is what I found
What are electrolytes?
An electrolyte is a substance that produces an electrically conducting solution when dissolved in a polar solvent, such as water. When applied to humans and health, it typically refers to sodium (Na+), potassium (K+), calcium (Ca2+), magnesium (Mg2+), chloride (Cl−), and is used for nerve signals and maintaining the right osmotic pressure in cells.
How does illness affect electrolytes?
Electrolytes are lost in sweat, including from fevers, environmental heat, and exercise. They can also be lost through diarrhea and vomiting- a big problem with bulimia.
Additionally, too much fluid can throw your electrolyte balance off, so if you’re following the advice to hydrate without taking electrolytes, you can make things worse.
What’s so bad about low electrolytes?
Your nerves will be worse at firing, leading to cramps, mental issues, and cardiac issues.
In extreme cases it can lead to spasms of the muscles in the throat (leading to difficulty breathing), stiffening and spasms of muscles (tetany), seizures, abnormal heart rhythms, and kidney failure (hypocalcemia, hypoatremia, hypokalemia). But you’re not going to let it get that far.
More speculatively, because calcium-based signalling is a key component in immune response activation, low calcium may weaken your immune system.
How speculative is this?
Not. Electrolytes are part of the standard routine in hospitals for COVID-19 and fevers in general.
Can I hurt myself with this?
Yes, but not easily. There is a level at which too much of any electrolyte is bad for you. My experience and the experience of many people I know is that you can tell by taste- electrolyte-enhanced water tastes amazing when you need them and unpleasantly salty when you don’t. Also barring certain specific problems like hypothyroidism, your body is pretty good at evening out your electrolytes as long as you give it the raw materials and time, so this is another reason to space out your fluid consumption.
The theory seems sound, what about the practice?
I looked for RCTs of electrolyte supplementation vs. not, but what I found was mostly studies of different types of rehydration therapies, always in children, and most for diarrhea induced imbalances rather than fever. The best I found was this meta-review showing isotonic IV fluid led to low sodium less often than low sodium IV fluid did
If you’re curious about the pediatric diarrhea studies...
How much do I need and when do I need it?
The literature was not very forthcoming on this, and I’m not a great person to ask because I put salt in my water by default. My folk wisdom is to add it to your water that you should also be drinking to taste.
Thanks to Eli Tyre for help with the research for this comment.
mostly studies of different types of rehydration therapies, always in children, and most for diarrhea induced imbalances rather than fever.
Any electrolyte losses due to having a fever for a few hours/days is not clinically significant which is why you can't find relevant studies. The body is capable of coping with a bout of pyrexia.
published in 1938: ELECTROLYTE BALANCES DURING ARTIFICIAL FEVER WITH SPECIAL REFERENCE TO LOSS THROUGH THE SKIN
Plain water is usually sufficient to maintain hydration during a a fever + a little salt if sweating a lot. ...
is something like pedialyte a reasonable OTC solution for electrolytes or would you suggest mixing out own concoctions?
EDIT: Changed blood oxygen numbers thanks to Jay Molstad Comment
What I would do if I had COVID-19? ( I am NOT a medical professional)
Ok. So you're sick. Maybe you have a fever and a bit of a cough. This may be COVID-19 and this may be something else like a seasonal flu. Even if you have COVID-19 the most likely outcome is that the symptoms are mild enough that you can deal with them at home. The South Korean Health Minister says 10%, so 90% you recover at home.
I asked my dad, a doctor (internal medicine). My blood oxygenation is usually around 92-93%. It can vary for a number of reasons. Anything under 90% is considered hypoxia, but the high 80s can be "normal" in a long time smoker.
The hospital is likely to be very busy and not have time for mild cases. Blood oxygenation of 92% does not warrant their attention. I'd give my doctor (or the emergency room) a call at 90% oxygenation. At 85% it's definitely time to go to the hospital (unless they tell you otherwise). Below 80% brings a severe risk of organ failure, so that's a life threatening emergency.
Use common sense - if your doctor is telling you one thing an a random internet comment is telling you differently, believe the doctor. Also, if your readings are going down rapidly, call your doctor. Don't drive if you're significantly impaired.
Take zinc at the first symptom.
Other people (Scott, PhilH, knzhou Cochrane Review) have gone into the science before and I don't have much to add to their research, but here's my adaptation for COVID-19 in particular.
My synthesis:
Caveats:
Should I take zinc prophylactically?
My first-principles, completely unverified guess is that if you take zinc all the time your body will adapt and it will become less useful. Also you will lose your sense of smell. I'm not taking it while in isolation, but I definitely would if I was a medic or grocery clerk right now.
I was under the impression that loss of sense of smell was primarily happening to people who take zinc intranasally. (I don't have numbers handy.)
My impression was that the effect of the zinc was supposed to be on the virus (or the virus's interaction with your cells), not on the body. Which (if true) would seem to imply that prophylactic use shouldn't cause adaptation.
This paper appears to be a discussion of a Cochrane review from 2011, and supports prophylactic use (and also generally supports use, and provides more info):
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3273967/
The 2011 version of the Cochrane review in question: https://www.ncbi.nlm.nih.gov/pubmed/21328251 / http://sci-hub.tw/10.1002/14651858.CD001364.pub3
(Irritatingly, there have been a number of subsequent versions of the Cochrane review, but several of them have been withdrawn, for reasons that are hard for me to interpret, although one at least involved an accusation of plagiarism from another meta-review on the same topic. It feels to me like there may be some kind of political fight over ownership of this Cochrane review.)
ALSO, while looking through Cochrane reviews, I found this one in favor of Vitamin C for
I have a few extra lozenges I can share, although if you're in the Bay Area, you'll have to drive to a different state to get them. Send me a personal message if you're interested.
Listing / summarizing some things I've seen elsewhere:
This general summary post by Sarah Constantin: https://srconstantin.github.io/2020/03/27/home-care-mild-COVID19.html
A post by SC specifically on "non-invasive ventilation", meaning CPAP and BiPAP machines (which some people may already have at home), with positive conclusions: https://srconstantin.github.io/2020/03/20/non-invasive-ventilation.html
A document by Matt Bell with information about chloroquine phosphate / hydroxychloroquine: https://docs.google.com/document/d/160RKDODAa-MTORfAqbuc25V8WDkLjqj4itMDyzBTpcc/
One of the most intriguing things I saw was about "proning": https://emcrit.org/pulmcrit/proning-nonintubated/
The author of that post is Josh Farkas, a pulmonologist (i.e. lung specialist) and assistant professor of critical care and pulmonary disease (i.e. lung disease.)
"Prone" here means a face-down lying position, the opposite of "supine" which means face-up. The author says "Typically we prone intubated patients." From context, I am reading "we" to mean his hospital / department, and "prone" to mean "rotate into the prone position for 6-18 hours per day." The commonality of this practice seems to vary among hospitals.
The post, however, is a discussion of proning for awake, non-intubated patients, and concludes that it appears safe and effective. There is a lot of uncertainty around how effective it is, but it looks to me like, if you have pneumonia and hospital treatment is not available to you, there is some evidence that -- perhaps counterintuitively -- you will breathe better lying on your belly, vs. on your back.
(The main counterpoint I have seen to this is that frequently moving around and changing positions is best. I can't tell whether the post is largely about patients who are too out-of-it to do that. I have seen it suggested that, if you're able, sitting up is better than lying down (I have no cite handy for this.) There seems to be overall agreement, at least, on this one point: lying stationary on your back for long periods of time is NOT good when you have lung problems.)
Idea I saw someone float:
If [a COVID-19] case becomes severe & ventilator access is limited, postural drainage is a thing I would be trying (seems low-cost & fits my models about what sort of thing should help). https://www.healthline.com/health/postural-drainage
Relatedly, if you're showing COVID-19 symptoms, I think I would recommend that you start lying on your chest if you can sleep and rest well in that position, using pillows for support as needed. I base this on an NY doctor working in a non-ICU COVID-19 unit who says:
Proning [i.e., having patients lay on their stomach] is now standard in our ICU and I tried hard to get my sicker patients to do it too to head off intubation. [...]
https://twitter.com/SepsisUK/status/1243236007346163712 [...]
[in reply to "Is proning something we can do at home to help with milder symptoms? My brother is short of breath but not at ICU level, should he try this?":]
Yes, can’t hurt, likely help
I only looked at these studies briefly, but they suggest that ARDS patients benefit from lying on their stomach:
Like Elizabeth, I remember reading somewhere that COVID-19 often starts in the upper respiratory track and becomes dangerous when it moves into the lungs. In line with that, one idea is to try to control the illness in the upper respiratory tract through sinus rinse/nasal irrigation (be sure to sterilize the water first). I haven't done much nasal irrigation, but I've found gargling with warm salt water to be really helpful for colds. This study found that simply gargling water for 15 seconds 3 times a day reduced upper respiratory tract infections by 36%! Breathing in steam or making use of a humidifier might also be helpful.
This pdf was linked from the 80K podcast. There are treatment instructions starting on page 8. There's also a section on what Traditional Chinese Medicine says you should do :P
There's also a thread on the slatestarcodex subreddit on what to do if you have a severe case and there's no room in the hospital. Another thread on that sub.
Find an RCT for COVID-19 treatment. This seems like a good compromise between "buy drugs from a sketchy foreign pharmacy and base dosage on a handful of papers" and "I dunno, my GP seems pretty on the ball".
One place I have found to find RCTs is https://clinicaltrials.gov/ . Normally I would verify the details of how to join but I assume they are busy right now. If you do try this, please report back.
Agree with the Vitamin D, C, and zinc. Also take nicotinamide riboside (a B3 variant) to raise PARP10 levels. (Recent paper on this):
https://www.biorxiv.org/content/10.1101/2020.04.17.047480v2
And don't forget to stagger around the neighborhood biting everyone... millions of movie fans have been waiting for this for decades.
Hello - this is the best resource I have found! I am currently on day 7 of presumed covid-19. I wanted to make some suggestions about viral pneumonia, which is often experienced by those who become ill when their conditions start to worsen. Viral pneumonia alone is not admissible criteria for EMD at this point.
My first sign that I had it was on day 3 if my illness, by far my most severe day. I was awoken by the sound of my own breathing, the sounds also caused my dog to scare and bark. I could hear purring/snoring/perculating/crackling from my lungs when I laid on my back, only when I was exhaling. Sometimes it sounded like a strip of explosive firecrackers going off. My PCP gave me no helpful information for palliative support or home remedies. She encouraged me to go to the ER without ever talking to me in person. They would have sent me home because I was never sick enough to be there.
Some things I found online to support at home care of pneumonia are:
Consuming a cup of regular coffee daily as caffeine is a bronchial dilator.
Avoiding all cough suppressants and instead take an expectorant. I took extra strength 12-hour Mucinex twice a day and was coughing up watery phlegm nonstop. Sorry for the visual.
Lying down prone and forcing yourself into coughing.
When sleeping, avoid your back and try to sleep on your right side as this is less pressure for your lungs and heart.
Use it cool humidifier or warm mist vaporizer.
Get up from bed and do light stretching every few hours. Take a few deep breaths and hold them for 10 seconds. Don't let your lungs become rigid.
If you are able to validate or research any of these suggestions, or add to the list, I think it would greatly help people. I am finally turning a corner and my pneumonia has not yet turned into respiratory distress. Thanks for the hard work you put into this.
Some intriguing stuff on hot/cold therapy here (https://youtu.be/EFRwnhfWXxo) and here (https://youtu.be/H1LHgyfPPQ8). I know nothing more than what's there. Also haven't read through every comment so forgive me if this is redundant. Take care!
{kind=link}
We’ve talked a lot about preparations and prevention, but statistically some of us, or people we care about, are going to actually get sick. What do we do once that happens?