So, how do you think Australia did, all things considered?
I think it's worth considering the federal and state governments separately.
The goal of zero transmission was and is clearly the best equilibrium to be in; we knew this early last year. Lockdowns suck but they work, and a fast+hard lockdown sucks a lot less than an epidemic. We went more than a year in Canberra between cases! The system works, and to be blunt if it was applied consistently COVID could have been eradicated by mid-2020... not that it could have been applied, but still.
Overall grade: C-, for an approach which was sufficient until betrayed by the combination of one particularly incompetent state and a federal government which turned down early access to Pfizer vaccines. D+ for policy, B for outcomes - we were adequate enough that good luck could make a difference.
I can't agree more. It is such a pity that what transcends to the news is mostly the negative stuff (especially about NSW and the slow vaccination) and not the fact that we have enjoyed 100% normal lives for the most part
My core reaction is, the very idea of a 22% decline in vaccine effectiveness per month doesn’t make any mathematical sense, until I figured out it meant a 22% increase in vaccine ineffectiveness. As in, if you are 99% effective in month one, and then you have a 22% ‘decline in effectiveness’ you would be… 98.8% effective. Or if you were 95% before, you’re 94% now. Which doesn’t sound to me like a 22% decline in effectiveness, even if true.
This is an extremely good point. I would absolutely not have guessed that's what they meant by a 22% decline in effectiveness. I would have thought "99% effective - 22% decline = 77% effective." Surely the authors knew this.
Do we all come together to form one big cominraty? Or should you be worried about the cominraties of getting vaccinated
Persistent typo here and elsewhere, of "cominraty" instead of "comirnaty"
After some poor marketing peon worked so hard to wedge the letters "mRNA" into the middle of their brand name.
Re. Australia, for some people this is hard to believe but in Queensland where I live, we have right now zero cases of COVID (there are cases in hotel quarantines, etc, but zero cases in the community). The army is on the border with New South Wales controlling that there are no people coming in (!). They took very seriously the zero-covid politics and I am sincerely impressed with how they managed this whole situation. I got my first shot a few days ago, and I am very happy about it.
Why is there no debate on "eradication"? Is the problem that the word sounds icky? Seriously, I don't get it.
Why don't we make a list of plans that would be logically sufficient to achieve The Obvious Win Condition and then "SELECT TOP 1, ORDERED BY plan.cost ASCENDING"?
Then the cheapest plan's costs give a reasonable "way to eradicate covid for a price" against we can compare "the human cost of more sick people from the disease itself plus the potentially years of bullshit costs in the form of mostly-pointless half-measures"?
My hunch is that eradication is cheaper than <gestures> "all of this". Am I wrong?
To plan eradication you would first need to estimate the effects of your various policies. The most promising policy at the moment is likely vaccines + prophylatic ivermectin. While you might argue that we need more studies to make sure that the prophylatic ivermectin studies replicate but it's likely still our best bet at the moment. It seems that for ideological reasons there's little interest in that.
Uttar Pradesh looks like it's making good progress towards eradication. The price in money in copying Uttar Pradesh's COVID policy isn't high.
50 years ago, if a region would have the success at fighting a disease like this, everyone would be willing to copy it. With our present institutions that's not the case.
Uttar Pradesh has almost a quarter of a billion people. I am very skeptical of claims that ivermectin made much of a difference there. I have been unable to find out how many ivermectin doses were sent out or used - hundreds of thousands? millions? But if we look at vaccination rates, about one quarter of the state have had one shot, and 5%, two shots. That's not enough to strongly affect infection rates, and I would be surprised if even that many people were using ivermectin.
They did have a severe outbreak in the second wave, like the rest of India, so an unknown fraction of the population would have antibodies. They implemented lockdowns, border control (I read that you can't enter the state without a negative PCR test), and other public health measures. UP has a BJP government (the chief minister is sometimes mentioned as a successor to Modi), and their supporters have been bragging about UP's successes compared to "Marxist" Kerala in the south, while their opponents have been saying that the figures are too low to be believed. I don't know who you should trust there. I notice that across the border in Madhya Pradesh, another mega-state with over 70 million residents, they also report extremely low case numbers.
It's definitely of interest to understand how things have unfolded in India, but I strongly doubt that ivermectin made much difference. At the very least we would need to know how many people there took it... My expectation is that the course of the pandemic in India is to be explained by a combination of public health measures, private caution, and perhaps natural herd immunity in some populations (like the Dharavi slum in Mumbai).
Ivermectin is relatively easy to produce for India while vaccines aren't. Them being supply constrained for vaccines doesn't indicate that they would face the same challenge for Ivermectin.
It's not easy to get information for Madhya Pradesh but what I get from Google indicates they also use Ivermectin.
border control (I read that you can't enter the state without a negative PCR test),
Border controls only help you when you have effective measures to reduce the case rate in your country. Them existing makes it more plausible that other measures in the country manage to bring the case rate down.
while their opponents have been saying that the figures are too low to be believed
When people said similar things about China's case rate being low, the general argument was that it's very hard to fake a case rate that low in a big country given an exponential disease.
It's plausible that Ivermectin isn't the whole story of why we see the numbers in Uttar Pradesh but it's one scenario that explains it that's consistent with what we see in the limited amount of prophylatic Ivermectin trials.
When it comes to Western public policy you could argue that we should have run highly powered trials to get certainty about whether or not Ivermectin has those effects after seeing what happened in India in May. If we would have done that we might have run a trial in 30,000 citizens in June/July and now have more reliable data.
However even in the scenario that the numbers from Madhya Pradesh and Uttar Pradesh are true and it's not due to Ivermectin, there's a credible scenario that those factors will also lead to lower infection rates in the US and Europe in the coming six months.
It seems part of the personal who measures cases in Uttar Pradesh is WHO personal which should make it harder to fake the case count.
Your link for Madhya Pradesh actually contains no data about ivermectin use there. The date marked on the graph is when India's national Covid protocols mentioned ivermectin (and various other medications). So far the only Indian states where I've seen reference to official use of ivermectin are Uttar Pradesh, Goa, and maybe Uttarakhand. Certainly there may be others.
My understanding is that in Goa, the health minister said they would make it available for all adults, then WHO's chief scientist (who is Indian) recommended not using ivermectin, and the national government removed ivermectin and other medications from the national protocols; and then Goa denied the policy.
In Uttar Pradesh, apparently ivermectin could be part of 7-day home isolation kits for people exposed to Covid or showing symptoms, but I have no data on how many such kits were issued, how many of them actually contained ivermectin, or how often the ivermectin was used.
Anecdotally, we can say that ivermectin has had widespread use in India in a decentralized way, as part of treatment for mild Covid or as part of a prophylactic regimen. But I remain very skeptical that it was widespread enough to significantly affect the course of the pandemic there.
40% of whitetail deer had a SARS-CoV2 infection by March 2021. https://www.biorxiv.org/content/10.1101/2021.07.29.454326v1 I'd expect it to be predominantly Delta in them too by now. Given the population and reproduction rate of deer, I'd expect the virus to keep circulating in deer indefinitely.
I love this response partly because it addresses something mechanistic about the world. Once the mechanism is raised it suggests things like: maybe the deer need vaccines? Or to be culled?
My central hunch for deer is that they are more exposed to humans (because of our garbage) than vice versa.
But like: listing out the aspects of the problem (deer, air travel, human trafficking, etc) and then listing sufficient sets of interventions to address all the aspects adequately... Is it really THAT expensive, compared with not eradicating?
It will be a different kind of eradication than smallpox eradication then, which is our golden standard for virus eradication. More like rabies management. Not zero cases forever, but small numbers of cases which are managed by vaccination where needed.
The Lancet had a "no-Covid" article, the UK has a "zero Covid coalition". But these predate the era of mass vaccination and the Delta strain.
Let us consider the known tools for suppressing the virus. One is restriction on human movement - quarantine, border control, lockdown. This worked for Australia and New Zealand before the Delta strain, but not any more.
Then there's antibodies: natural immunity in those who already caught the virus; vaccination; and herd immunity from a population full of antibodies, making effective transmission difficult.
The major western vaccines were touted as good for preventing transmission and infection. But at this point, their main unequivocal virtue lies in preventing serious illness. To an unknown degree, vaccinated people can still get infected and can still infect others. This, along with reluctance to get vaccinated in a significant portion of the population, is why masks and other such measures have returned.
Given that social resistance to vaccination and to continued restrictions, an optimal strategy cannot assume 100% consent and participation. Perhaps the way it will play out, is that vaccination and other public health measures will play the main role, and the remaining role will be filled by natural herd immunity building up among the unvaccinated.
We could easily update our vaccines to be more effective against Delta. It's just about swapping the sequence. We could test additional vaccines against targets besides the spike protein and see whether it improves immunity.
We could run highly powered studies for substances such as ivermectin. The same goes for the other six treatments on the FLCCC preventive protocol.
We recently saw cases in states like the UK go down for reasons we don't fully understand. If we would do more science to understand it that might give us additional ways to fight COVID.
I expect there's a lot to be gained by improving air quality, both air filters and humidity control.
I assume that most people are imagining eradication plans using [something close to current tools], and see solving the required coordination problems as a non-starter in that context.
I think that for eradication to be a realistic prospect you'd need a plan which a country could implement unilaterally with significant chance of long-term success. That seems to require new tools. I don't have a good sense of the odds of finding such tools, or the costs involved (either in research or implementation).
It would still be nice to see some informed discussion exploring the possibilities.
Free donuts! (And, with lower confidence, free money.)
I especially like how the Kristy Kreme advertising campaign rewards people who got vaccinated any time in the past. This reward structure motivates getting vaccinated early. This is the opposite of incentivizing the act of getting vaccinated itself, which sometimes motivate holdouts.
Or at least, that’s what the pharma companies that have every financial incentive acting against this are revealing they believe.
The pharma companies have a financial incentive that everyone gets vaccinated every six months. Adapting vaccines to be better protective against variants makes that less likely.
The pharma is not a single company. If one company develops a single-shot vaccine that is effective against all variants forever it would sweep the competition
If one company would update to the Delta spike protein the other companies would simply also update to Delta. There's no way to get a competetive advantage for it.
Given political pressures COVID-19 vaccines can't be sold at a price that corresponds to the value they provide and currently all produced vaccine doses seem to find buyers.
You also can't run studies to prove that your vaccine that's more resilient to variants actually has that property before those varients arise, so it's unlikely that market competition would work the way you assume.
It's worth noting that even if there's little practical difference that comes from updating to delta that likely would still be a marketing advantage. Not going for that marketing advantage shows how little the involved companies care for it.
There seems to be a lot of misunderstandings (or partial understandings) of the "spike protein" in the vaccines. It's not a full reproduction. https://www.medpagetoday.com/special-reports/exclusives/91648
From the early stages of COVID-19 vaccine development, scientists sought to target a SARS-CoV-2 protein that was least likely to cause ADE. For example, when they found out that targeting the nucleoprotein of SARS-CoV-2 might cause ADE, they quickly abandoned that approach. The safest route seemed to be targeting the S2 subunit of the spike protein, and they ran with that, wrote Derek Lowe, PhD, in his Science Translational Medicine blog 'In the Pipeline.'
It sounds like Delta only has one change to the S2 subunit, and there was some expectation that it would change less than S1 since vaccine development began. https://www.news-medical.net/news/20210628/Why-SARS-CoV-2-delta-variant-is-more-infectious.aspx
https://www.frontiersin.org/articles/10.3389/fimmu.2021.637651/full#F1
The spike protein of B.1.617.2 variant contains nine mutations in the S1 subunit and one mutation in the S2 subunit. In the S1 subunit, five mutations are present in the N-terminal domain containing binding sites (epitopes) for neutralizing antibodies. In addition, two mutations are present in the receptor-binding domain of the S1 subunit, which is known to influence antibody-mediated neutralization and infectivity. Among the three remaining mutations, two are known to increase angiotensin-converting enzyme 2 (ACE2) binding, viral replication, and spike protein cleavage at the S1/S2 site.
I'm not going to pretend that I know more about this beyond the surface-level (no pun intended) but it seems to me that if there's only one mutation, then the I would expect a small commensurate change in vaccine effectiveness (which seems to be what we've seen so far).
TV invents a disease you think you have
So you buy our drugs and soon you depend on them
Pain is in your mind, got you coming back for more again and again and again and again
Gonna rip you off, rip you off!
Doctor says you need surgery now
You're feeling good, 'til the side effects fuck up something else
You're ensnared by the medicine man paying up the ass again and again
Gonna rip you off!
This is always a real risk, but I hear it with everything. Yes, we have the FDA, but we also have regulatory capture. True. But we also live in a, at times, wonderfully litigious society.
I know the Pharma companies got some legal immunity, under PREPA (as I understand it, also not an attorney) but it doesn't seem as airtight as I thought. https://en.wikipedia.org/wiki/Public_Readiness_and_Emergency_Preparedness_Act#Liability_protection_and_consolidation_of_oversight
PREPA removes the right to a jury trial for persons injured by a covered vaccine, unless a plaintiff can provide clear evidence of willful misconduct that resulted in death or serious physical injury. The act instructs the HHS secretary to write regulations "that further restrict the scope of actions or omissions by a covered person" that constitute willful misconduct.
A plaintiff whose claim is subject to PREPA can sue the defendant only in the United States District Court for the District of Columbia. For such a civil action, PREPA requires the complaint to be pleaded with particularity, verified under oath by the plaintiff, and accompanied by an affidavit from a non-treating physician to explain how the covered countermeasure injured the plaintiff, as well as relevant medical records.
And Acts can always be repealed by Congress, or I suppose it could also be found unconstitutional by the Supreme Court.
If it ever came out that Pfizer, Moderna or J&J were creating vaccines such that they could only be effective if given every six months (and it's hard for people to keep secrets like this for long), I feel very certain that PREPA would be litigated or repealed or found unconstitutional.
(edits: spelling, grammar).
I'm not going to pretend that I know more about this beyond the surface-level (no pun intended) but it seems to me that if there's only one mutation, then the I would expect a small commensurate change in vaccine effectiveness (which seems to be what we've seen so far).
There's an idea called evidence-based medicine that's popular in medicine lately. According to it one seeks to not extrapolate based on arguments like that but looks experimentally at what actually happens. What happens is:
Sera from individuals who had received one dose of the Pfizer or the AstraZeneca vaccine had a barely discernible inhibitory effect on the Delta variant. Administration of two doses of the vaccine generated a neutralizing response in 95% of individuals, with titres three- to fivefold lower against the Delta variant than against the Alpha variant.
Moderna/Pfizer don't make any promises that the vaccine protection is going to hold forever. An argument that they could have developed a better product is very far from showing that they have injured plaintiffs.
That said, developing better products isn't free. It takes research. Updating the vaccine to Delta costs money. There's no legal obligation to do that.
We're both speculating based on different data. You're citing an in vitro study using sera from individuals with one or two doses, and there's some amount of mechanistic speculation in terms of how decreases in neutralization response and titers changes the ultimate outcome, which is case severity of vaccinated people exposed to Delta compared to unvaccinated people (at least in my mind). So far that still seems very positive.
Thinking in more of a comp sci way, it strikes me that there could also be a problem of over-fitting for a specific variant of the s2 subunit. Say Pfizer and Moderna thought about changing the mRNA to specifically match the Delta s2 subunit, but maybe they're anticipating a world where the next more contagious strain doesn't contain that s2 subunit mutation? Or maybe, like you suggested, it is just a cost-benefit thing.
Moderna/Pfizer don't make any promises that the vaccine protection is going to hold forever. An argument that they could have developed a better product is very far from showing that they have injured plaintiffs.
Maybe. But it's not that far. If they really had designs somewhere to make a vaccine that would last substantially longer and they scrapped them in favor of one that lasts 6-12 months... I just think the probability of the IP for the better designed being concentrated only in a few companies and not independently discoverable by other people is low, and the probability that it could be kept secret for months or years is low. The probability of the Frank Azars of the world hearing about that and taking a shot at litigating it for a piece of a very very large settlement seems high (low-risk, high-reward), but more likely I think Congress would amend or repeal PREPA under that circumstance and open the floodgates of lawsuits.
Say Pfizer and Moderna thought about changing the mRNA to specifically match the Delta s2 subunit, but maybe they're anticipating a world where the next more contagious strain doesn't contain that s2 subunit mutation?
When we do influenca vaccines we use multiple targets then just one to be able to vaccinate against multiple strains. Even if you assume that only 50% of future variants include the Delta spike protein you could give 50% alpha spike protein and 50% delta spike protein in your vaccine.
Ideally, I would expect a vaccine that's designed to be resistant against mutations to go the RaDVaC way of targeting peptides in different proteins of the virus to prevent any single mutation from removing the protection.
Of course that means that you need to run studies to validate targets.
If they really had designs somewhere to make a vaccine that would last substantially longer and they scrapped them in favor of one that lasts 6-12 months.
Things are more complex then that. If we believe the Moderna people they essentially decided on the vaccine they wanted to produce within days after the Chinese finally decided to publish the full sequence including the full spike protein with it's furin cleavage site.
Given that it was important to have a vaccine as fast as possible that was a reasonable approach. Creating a vaccine that's more resistant to mutations takes work. The decision to stay with that vaccine instead of investing into creating a better version is an economic one for which you couldn't persue a company in front of a court.
Given that it was important to have a vaccine as fast as possible that was a reasonable approach. Creating a vaccine that's more resistant to mutations takes work.
Just doing some quick searching, it doesn't sound like that's the decision that they're making. At the moment is sounds a little more like a toss up between a third shot and a delta-specific one.
The decision to stay with that vaccine instead of investing into creating a better version is an economic one for which you couldn't persue a company in front of a court.
I'm not sure that Ralph Nader, for example, would entirely agree. Unsafe at Any Speed is analogous to the extent that car makers were optimizing for one set of conditions (cars that would get you laid) rather than another set (optimizing for cars that are less likely to kill you). What you're saying here (correct me if I'm way off) is that vaccines were optimized for ease of manufacture and dissemination rather than providing more comprehensive long-term immunity, and that financial incentives are now against pharma companies optimizing for more comprehensive long-term immunity...
Our legal system (mostly legislative in this case) was still able to deal with this and car makers now are required meet safety standards.
But that being said I'm all for doing what can be done to make incentives less perverse. Maybe find someone biologically-savvy and bureaucratically-minded to draft an initial set of vaccine quality improvement guidelines. Like a Deming wheel but applied to increasing vaccine efficacy, and if you get federal money you have to follow. Those are hard problems to solve.
At the moment is sounds a little more like a toss up between a third shot and a delta-specific one.
In a reasonable world the change to a delta-specific one would have happened months ago.
What you're saying here (correct me if I'm way off) is that vaccines were optimized for ease of manufacture and dissemination rather than providing more comprehensive long-term immunity
No, I think the choices were awful for the goal of ease of manufacturing. The goal was getting approval to bring the vaccines to market as fast as possible (the prelimary approval type).
In a pandemic, it's good to have vaccines available sooner then later. That's a different goal then optimizing for cars looking good.
Is it really the case that any company is not trying to update to the Delta spike? how do we know that?
Then, saying that the other companies would not get any competitive advantage for that will depend on the time frames. If one company can release vaccines against new variants quicker than the rest, they would have an advantage there.
You also can't run studies to prove that your vaccine that's more resilient to variants actually has that property before those varients arise, so it's unlikely that market competition would work the way you assume.
That's a fair point, though you can show at least in theory that a vaccine is effective against all variants that have appeared so far.
Your statement last week was correct: there is no known danger of vaccines during pregnancy. There is general advice to avoid them because of purely theoretical dangers.
I share your skepticism regarding mandatory boosters for everyone. Hopefully at some point people will be given additional options, like:
https://www.cnbc.com/2021/08/20/astrazenecas-antibody-therapy-prevents-covid-study-shows.html
Or maybe we add a layer of abstraction - once everyone has had their first N shots (where N is the number of shots needed to get us to normal) we mandate semiannual checkups and it's up to the physician to evaluate whether you need a top-off (and if so what kind). Sort of like safety and emissions inspections for cars - we mandate that cars get checked regularly, and the mechanic decides what's needed to bring the vehicle into compliance.
The link to "Israeli data" is wrong; it goes to the tweet by @politicalmath showing the Houston graph you inlined later.
typo: An argument against weaning masks on the margin, and
should be
An argument against wearing
giving away free donuts as an incentive to vaccinate against covid specifically, well... do all marketing people go to hell?
On using water for lawns. Having moved from a megapolis to suburbs (and caring not at all about how my backyard looks, I'd rather have it paved over), lawns are essential for the general health of the environment, and watering them is essential to keeping them alive in a painfully obvious way.
You let lawns die, you get mud. Mud gets shifted to the road, where it dries and becomes sand and dust. Sand and dust get lifted by cars and cover everything. If you want to see this in action - visit St Petersburg in Russia, where they parked on all of their lawns and killed them, and now everything is covered in 1/8" of sand.
Once your lawn is dead, it takes much more water to rebuild than it would take to maintain.
How long does it take a lawn to die? The request in this case was to leave them for a week when there'd likely be a thunderstorm, so I'm guessing it's not a serious worry in this case. (But it might be one in other cases where there's a limited supply.)
You let lawns die, you get mud. Mud gets shifted to the road, where it dries and becomes sand and dust. Sand and dust get lifted by cars and cover everything. If you want to see this in action - visit St Petersburg in Russia, where they parked on all of their lawns and killed them, and now everything is covered in 1/8" of sand.
Once your lawn is dead, it takes much more water to rebuild than it would take to maintain.
Zero-scaping Xeriscaping is a thing - developing a lawn with succulents, packed rocks, artificial turf, etc. such that it's solidly developed yet requires little or no water. It's increasingly popular (in large part due to water use regulations) in California.
I strongly agree that lawn care is a terrible use of water when there’s a limited supply, but the way we figure such things out in a sane world is we charge more money for water and if desired or needed give people a credit to avoid distributional concerns. Yes, I know, don’t make you tap the sign, go write on the blackboard, etc etc.
In a sane world, people voluntarily help each other, especially during emergencies. Charging more for basic necessities hurts the most vulnerable.
Do you mean that if I give you a perpetual $20 coupon to buy bottles of water and then increase the price by $20 you have lost something?
Do you mean that when you said "charge more for water" you meant "charge more for water , but some people also get their water free"?
If you didn't make libertarian- sounding sideswipes at all, and it would also help if your turned them into nuanced arguments.
OK...but I don't see how that helps. It might be Zian's idea that poor people obviously do or should get water vouchers...but is it Zvi's idea? Zvi brief statement sounded like pure pay-or-go-to-the-wall libertarianism. Perhaps that was only because it was brief, perhaps not.
OK...but I don’t see how that helps.
Helps with what? It's relevant in that when you asked Zian "do you mean that when you said...", Zian had not said that thing. It seemed to me that you were talking to Zian under the impression that they were Zvi, and this seemed worth pointing out. It seemed like it might help avoid people talking past each other, for example.
It might be Zian’s idea that poor people obviously do or should get water vouchers...but is it Zvi’s idea? Zvi brief statement sounded like pure pay-or-go-to-the-wall libertarianism.
I don't claim to know exactly what Zvi thinks, and I don't feel like getting into the weeds on this any more than it seems he does. But...
You've made three comments in this thread so far, and in not one of them have you acknowledged that Zvi included the phrase "if desired or needed give people a credit to avoid distributional concerns".
I feel like that phrase is obviously relevant to your concern, even if you don't know exactly what he means by it and/or what you think he means doesn't fully address your concern. And I think failing to acknowledge it reflects poorly.
(I would say that Zvi spends 18 words on libertarian content, "the way ... for water", and 12 on addressing a possible failure mode of the libertarian content, "if desired ... distributional concerns". It seems to me that calling this "pure pay-or-go-to-the-wall libertarianism" is frankly ridiculous.)
Great news, everyone. The Pfizer vaccine has been approved. Woo-hoo!
It will be marketed under the name Comirnaty. Doh!
(Do we all come together to form one big cominraty? Or should you be worried about the cominraties of getting vaccinated, although you should really be orders of magnitude more worried about the cominraties of not getting vaccinated? Did things cominraty or was there a problem? Nobody knows. Particle man.)
My understanding is that if a doctor were to prescribe the vaccine ‘off label,’ say to give to an 11 year old or to get someone an early booster shot, then they could potentially be sued for anything that went wrong, so in practice your doctor isn’t going to do this.
A reasonable request was made that my posts contain Executive Summaries given their length. Let’s do it!
Executive Summary of Top News You Can Use
Also, assuming you’re vaccinated, Krispy Kreme is offering two free donuts per day from August 30 until September 5.
Now that that’s out of the way, let’s run the numbers.
The Numbers
Predictions
Prediction from last week: 1,000,000 cases (+14%) and 8,040 deaths (+45%).
Results: 935k cases (+7%) and 7,526 deaths (+35%).
Prediction for next week: 950k cases (+2%) and 9,400 deaths (+25%).
I was confused how there could be such sharp peaks in other countries. It looks like we won’t get one of those. The trend lines seem clear, and it looks like we are approaching the peak. It would be surprising if we were still seeing increases week over week by mid-September, with the obvious danger that things could pick up again once winter hits.
Deaths
Deaths continue to lag cases. News was slightly good, so adjusting expectations slightly in response. Peak should still be a month out or so.
Cases
Vaccination Statistics
How much will full FDA approval matter? Survey says not much.
I am more hopeful than this, and expect more than a 10% increase. Some of this will be people for whom this really was the true rejection. Other parts of it will be as mandates are handed down and people anticipate further mandates.
Vaccine Effectiveness
I continue to find this very telling in terms of vaccine effectiveness versus Delta:
The argument is simple. The Delta vaccines are designed and would be easy to get approved, yet there has been no move to manufacture them quickly. The only reasonable explanation for this is that there isn’t actually much if any difference with the old vaccine. Or at least, that’s what the pharma companies that have every financial incentive acting against this are revealing they believe.
A new paper on vaccine effectiveness concurs (preprint).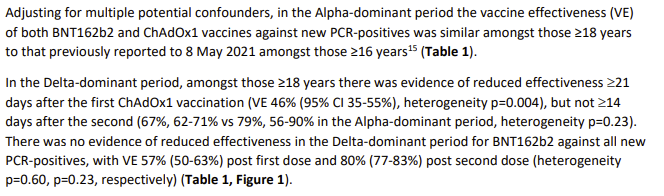
I will for now accept the principle that a single dose provides substantially less protection against Delta than Alpha, but this is another data point that Delta isn’t different from Alpha once you get your second shot. I always find maddening the ‘confidence intervals overlapped, so nothing here’ reaction to differences like 67% vs. 79% – yes, you can’t be confident in that, but that’s mostly saying your study was underpowered, since that’s the kind of difference one would expect if there was a difference, and again, the word evidence does not mean what they think it means.
The paper’s findings then get worse, if you believe them, claiming rapid reduction in effectiveness over time.
They then go on to say this, which given how vaccinations were timed seems likely to be confounding indeed:
There’s no one good money quote on it, but the findings robustly say that vaccinated people’s cases tend to be lower viral load, less dangerous and less severe.
Looking at their section on statistical analysis, they’re doing some of the necessary and reasonable things but I can’t tell if it’s enough of them. Such studies are better than nothing if treated with caution, and this seems like a relatively well-done one, but I’m still more focused on the population numbers and what makes the models work out.
When I see things like this:
My core reaction is, the very idea of a 22% decline in vaccine effectiveness per month doesn’t make any mathematical sense, until I figured out it meant a 22% increase in vaccine ineffectiveness. As in, if you are 99% effective in month one, and then you have a 22% ‘decline in effectiveness’ you would be… 98.8% effective. Or if you were 95% before, you’re 94% now. Which doesn’t sound to me like a 22% decline in effectiveness, even if true.
Israeli data continues to suggest extreme fading of vaccine effectiveness if you look at it naively, along with yet another reason to, as post puts it, proceed with caution.
New data from Denmark:
One presumes that the improvement against hospitalization in Pfizer is a data artifact or failure to control for something or some such, which shows how easy it is to get misleading results, especially since infection went the other way. And this big Pfizer versus Moderna difference against Alpha isn’t found elsewhere, which makes me think that once again there’s confounding going on all over the place.
Here’s a thread analyzing some of the results, and takes the declining protections and other study data fully seriously, putting the burden of proof on finding something specific that is wrong with the studies, and otherwise taking their results and details seriously and forming the model around that. As usual, the broader context of what such results would mean for all the other data we see isn’t incorporated – but again, I don’t see anyone doing that.
Here’s another good long thread explaining what vaccine effectiveness means then listing lots of different findings and real world results. Putting them all together like that makes it striking how much the different numbers don’t agree if you take them all at face value.
I continue to think that the decline in vaccine effectiveness over time is in large part a mirage, and for practical purposes the decline is relevant but small.
This week’s representations of how those vaccines are doing, after having vaccinated about 70% of adults and most of the elderly.
Virginia offers a dashboard:
Doesn’t look like vaccines are losing effectiven
Houston, via PoliMath:
And another:
And another:
That’s disappointing at face value since it’s only a 90% reduction in deaths but after correcting for age it would look a lot better. Weird that so much of the vaccine advantage here seems to be coming after hospitalization.
A worry is that the studies are selecting for ways to show vaccinated people are at risk, and another worry is that the real world statistics being reported are selecting for showing that the vaccines are super effective, because they are the same information but the Official Story is on two contradictory propaganda tracks and is pretending not to notice that this is a physical world question with a correct answer (whether or not we are confident we know what it is).
Anecdotal in Tampa, Florida
Here in New York:
Meanwhile also this:
Note that yes, we are excluding the first wave infections here as per her follow-up note, but note the graph and adjust accordingly, and I think the point stands.
That does bring up that UK cases are clearly rising again, so we can no longer use that as an important signpost that things will turn around rapidly and that will be that. If anything, it’s now making the case that such a turnaround is unlikely. I don’t know of anyone who has offered an explanation other than a shrug for the decline followed by a reversal here.
As for the reinfections versus vaccine effectiveness, my hypothesis is that this is not a case of ‘immunity from infection holds up but vaccine immunity is losing ground.’ Remember when we were worried that natural immunity faded with time but vaccines solved that problem? The actual difference is in the methods of observation. When similar observational methods are used, we seem to get similar results.
How infectious are breakthrough cases? We now have two studies for that. They found that vaccinated people who get infected are still infectious, but their viral loads are substantially lower, so this was what we previously expected. And also they clear the virus faster, which was also expected.
Weirdly, they’re two different studies that find the two different results, although depending on how you measure, fading quickly implies lower average viral loads, so the results are compatible with the graph and it’s possible what we’re seeing is a shorter period of infectiousness rather than less at the peak. That seems unlikely to be the whole effect to me, but could easily be the majority of the benefit.
How much comfort that brings depends on the situation and on what you previously believed. If you’re as bad at this as the CDC and were saying the vaccines ‘prevent transmission’ full stop and now that they ‘don’t prevent transmission full stop’ it gets confusing.
Vaccine Hesitancy and Mandates
Formal approval is in, so here… we… go.
I saw this about one minute after I saw the FDA had approved the Covid vaccine, perhaps someone planned something in advance for once:
On her first day on the job now that The Worst Is Over, our new governor lays down the law:
She also raised New York’s total death count by 12k, which once again highlights that maybe Cuomo went down in a similar way to Al Capone (who was indeed guilty of tax evasion).
Although she’s also mandating ‘ethics seminars’ so you win some and you lose some.
LSU is going to mandate vaccination or a negative test for all fans at Tiger Stadium.
Whereas the University of Georgia is going the other way.
Here’s the owner of the Dallas Cowboys:
Who else we got (WaPo)? They found CVS Health, Deloitte and Disney, but so far, not an impressive set of additional mandates. It seems not many were standing by ready to go.
Delta Airlines is charging unvaccinated employees $200 a month extra for health insurance, on the very reasonable premise that every hospital stay for Covid costs them an average of $50,000 and they end up in the hospital for Covid more often. Insurance companies can’t do this, but it seems corporations employing you can do it.
NYPD has threatened to sue if the city attempts to implement a mandate.
Texas Governor once again mandates against vaccine mandates, this time ensuring it applies despite FDA approval.
When you’re fully anti-vax, you’re anti-vax, and it’ll be hard to tell you different, as Donald Trump learned:
Others are less fully anti-vax, but still unvaccinated, thanks to various ways we botched things.
As Ranu notes there are two distinct things here. First, we botched the logistics, and could have done much better if we’d made sure to beware trivial inconveniences that aren’t always trivial. Second, our authorities are untrustworthy so people don’t trust them. This is framed here in the standard blue-tribe way as ‘the system fails such people and they remember the legacy of all that’ with it being ‘hard to make up’ during a pandemic, rather than the simple ‘these people lied about the pandemic over and over again’ model. Both are presumably relevant, but my guess is that handling the pandemic in a trustworthy fashion would have largely solved both problems. Yes, such people will absolutely ask why you weren’t helping them before, but that’s different from turning your help down if you’re here now.
One aspect of vaccination decisions is that patients in America do not pay for their health care. Almost everyone who can get it has health insurance because if you don’t the medical system bills you personally and attached some number of extra zeros to the bill because they can, so you can’t opt out. For a while, they even waved ‘cost sharing’ on Covid, so you didn’t even pay the fraction you normally pay, but that’s increasingly no longer true. Would be good if more people knew. Incentives matter, but only if people are aware of it. One could note that this policy could be taken farther, if the government permitted this, so we’re doing mandatory mandates with one hand and mandatory massive subsidies to those who don’t follow those mandates with the other.
State employees, you will get vaccinated as many times as is legal, or else.
This is an explicit ‘everything that is not forbidden is mandatory, and everything that is not mandatory is forbidden’ rule. You can get exactly this many shots at exactly these times, and you either get them or you’re fired. There’s no concept of a booster that is optional, based on someone’s situation, and the full mandate applies to teleworkers.
This is where things are going to be tricky. Requiring ‘full vaccination’ so far has been simple. You get two shots and that’s it. Now there are signs that this in many places is going to morph into getting periodic boosters with different places (at a minimum, nations, Austria and Croatia are already setting expiration dates) having different requirements, and those boosters will have a much less slam-dunk risk-benefit profile.
I will happily take the third shot without any need for outside incentives, but it is a very reasonable position to not want the third one, and it seems likely that requiring boosters will have far less robust support than requiring two shots.
A cheap shot, but I think a necessary one so putting it here anyway, without any need for further comment.
One can definitely say shots fired:
Masking, Testing and NPIs
This is nuts, actively counterproductive on every level, and what must be fought against:
To be fair, it is only required ‘when social distancing is not possible,’ most of the time this will definitely apply, and I assure you that it’s always possible.
It’s always adorable when people think the constitution is a meaningful limiting factor, and all recursive mandate sentences are fun.
In practice, this is technically true, but there is a known way around it known as withholding federal funding. And another easier way around it, called ignoring the constitution, since presidents mostly do what they want without any actual legal authority under the constitution and mostly no one calls them out on it. Eviction moratorium, anyone?
If you’re in NYC and either old or immunocompromised, make sure you know about this:
You can also buy one at the pharmacy, although not like in Europe where the tests are super cheap and abundant. FDA Delenda Est.
Also, a periodic reminder that the reason younger children can’t get vaccinated, which in practice is causing super massive freakouts although there’s almost zero risk there, is that the FDA moved the goalposts to require additional data. Thus we almost certainly won’t get this before the end of 2021, and I’d double check but this market sure looks a lot like free money.
Here’s a graph of how afraid people have been over time:
The lack of an increase in fear over the winter surge is the most surprising thing here. Otherwise it all makes sense, with fear going down when things were improving, then fear starting to go back up as cases rise. Fear isn’t a perfect proxy for the private control system, but changes in fear likely predict marginal changes in private actions and we’re back at levels similar to April.
Here’s a survey on activity:
As one would expect by now, vaccinated people are taking more precautions than unvaccinated people. Almost half of vaccinated people are ‘avoiding people as much as possible’ and they’re claiming it’s because of the pandemic. However I share Nate’s skepticism here minus the word ‘little’ because math:
Perhaps ‘as much as possible’ means until one is hungry, or has somewhere to go. It’s on the margin.
Study does some modeling and finds that according to its model masks work, ventilation works even better.
From the study:
Filters win out here over windows, if one has to choose, and of course if possible you’d do both. Also you can’t cheat on the windows, you gotta actually leave them open. When we’re considering actions like mask mandates or shutting down living life entirely I find it odd that people worry about energy costs this much, but there you go. Also fresh air remains a Nice Thing. As always, one must be highly skeptical when translating such results into predictions for actually preventing cases.
A potential issue with price controls:
An argument against weaning masks on the margin, and a good question about presenting that argument.
I found the tweet more compelling than the full post. Getting into the details mostly highlighted places I disagreed with Bryan.
Booster Shots
Governor of Texas gets a third shot as a booster. I have no issue with people in high positions getting superior medical treatment when there’s a supply or resource shortage, but meanwhile we have vaccines expiring in some places. That’s from Scott’s post with further comments on the topic of FDA Delenda Est, which is interesting but inessential.
The new argument against booster shots is that they… might cause us to produce too many antibodies against Covid, and then maybe Covid mutates and the antibodies become dangerous or unhelpful because they’re overtrained? When it’s not Officially Sanctioned even antibodies are labeled bad, it seems. Meanwhile this is doubtless supposed to make people worried about Delta, but this worry definitely does not apply to Delta, and an additional customized booster would be necessary in the cases being described either way. Don’t worry, such arguments will go away once the Official Sanction comes down, which is coming soon.
Meanwhile, an argument for booster shots is that the first two doses were so close together that they count as a primary immunization, claiming it looks like this:
Which is so insane it doesn’t even bother putting any impact from the second shot into the chart at all, and puts the peak of the ‘primary’ response more than halfway down the graph when it’s almost fully effective. There’s obvious nonsense available on all sides.
Think of the Children
We really do have a large class of Very Serious People, with a lot of influence on policy and narrative, who think that living life is not important, that the things you care about in life are not important, and that our future is not important, because saying the word ‘safety’ or ‘pandemic’ should justify anything.
This week’s case in point, and like my source MR I want to emphasize that this is not about the particular person in question here.
If anything, I’d like to thank Dr. Murray for being so clear and explicit. If you think that safety trumps the need for love, for friends and for living a complete life in general, then it’s virtuous to say that outright, so no one is confused.
In case you think she doesn’t mean that (or that others don’t mean that), no really, she does:
Ellie Murray does not believe that school is terrible, so she is simply saying that the claimed benefits of school are not important relative to the marginal impact of schools on Covid-19.
That reply was one voice in a chorus, as the replies are what you’d expect and rather fun to read through. Nate Silver sums this up well:
There was also a side debate over whether school is the future of our children and our children are our future, or the alternate hypothesis that children are also people and school is a prison and dystopian nightmare. The thing to remember is that this view is not driving most of the anti-school rhetoric. Such folks mostly think school is vital to children, but don’t care.
Yes, I was aware, and I’d rank my concerns regarding school in this order:
But yeah, we can beat that take this week, because the The Times Is On It:
Technically I’m sure it is true that masks represent an ‘educational opportunity’ in the sense that whenever anything happens you can use it as an opportunity to learn. The main such opportunity is to learn about those making the decisions.
In Other News
Have you tried using a market clearing price? No? Well, then.
I strongly agree that lawn care is a terrible use of water when there’s a limited supply, but the way we figure such things out in a sane world is we charge more money for water and if desired or needed give people a credit to avoid distributional concerns. Yes, I know, don’t make you tap the sign, go write on the blackboard, etc etc.
Biden still hasn’t appointed anyone to head the FDA, but at least he floated a name. The name is someone who said that living past 75 is a waste, but hey, pobody’s nerfect, right?
Obama literally hired a doctor to ensure everyone was vaccinated and safe and his party was still a huge issue, so now everyone in Washington is afraid to throw parties. Also for other reasons, I’d imagine, but those are beyond scope.
A calculation of whether the benefits of exercise in a gym exceed the risk of Covid finds that it very much does in her case. Often the choice really is between going to the gym or not exercising. Her calculation did depend on the lack of other people in the gym, however, so if the gym had sufficiently more people in a tight space the calculation could have gone the other way. She has a spreadsheet you can play around with if you’d like to explore this more.
Denmark gives up on the mystical ‘herd immunity.’ Usual misunderstandings here but I suppose this is better than the practical alternative of not giving up.
Thread reminding us that the control system has many facets, and they work together at least additively and often multiplicatively. You don’t need any one factor to control the virus or get you mystical ‘herd immunity’ on its own, you care about the combined effects.
Zeynep reminds us that plastic barriers are likely to be net harmful because they interfere with airflow. I got this one wrong early on, same as everyone else. The key is to update.
Monoclonal antibodies are free and effective against Covid, but few people are getting them (WaPo).
From MR: You can get flown home if you get Covid while abroad, but you’ll need a special service.
Germany moves to using hospitalizations as the primary measure of whether Covid is under control. This makes sense for policy, since what matters is whether the hospitals are overwhelmed and whether people are sick and dying.
Australian stockpile of AZ continues to grow, over 6 million doses (via MR).
Australians who are vaccinated overseas can register that vaccination, but only if the vaccine was approved in Australia at the time of vaccination. Which was not a rapid process.
I like how transparently the ‘at the time’ restriction is purely harmful. No fig leaf.
Also via MR, due to continued Covid restrictions down under, they shot dogs due to be rescued by a shelter to prevent shelter workers from travelling to pick them up. Meanwhile, they’ve uncovered people getting fresh air. It’s becoming an epidemic of fresh air getting after 200 days in lockdown.
But good news, if you’re fully vaccinated, you’re about to get new freedoms!
So, how do you think Australia did, all things considered?
Poison control is lonely work. Not many people call, and when they do, it’s usually something like ‘I took prophylactic Ivermectin that was intended for animals, thinking that was a good idea.’ We have some news.
General warning for anyone who needs it: Animal formulations of a given medicine are often different from the human version, and could be highly dangerous to humans. Do not perform this regulatory arbitrage assuming that the two things are the same.
Also, this:
They didn’t know the two things were different, and it’s a perfectly reasonable hypothesis that a thing could be vastly cheaper and easier to get if you can do an end run around the FDA, or around pharmacists earning praise for refusing to fill prescriptions for Ivermectin. This simply was not one of those times.
Also note the numbers. One individual was told to ‘seek further evaluation,’ and 85% of the cases were mild. The definition of ‘mild’ can be whatever people want it to be, but if it’s ‘no need to seek further evaluation’ it seems like there were six poison control calls out of eight total calls? I’m guessing it’s higher than that, and please if you decide to take Ivermectin make sure you’re sourcing and dosing it safely and properly, but this isn’t an epidemic of cases, and this was going around enough it felt important to point that out, even if I’m highly skeptical that Ivermectin does anything useful.
Rob Bensinger offers his advice on what to personally do about Covid. Not endorsed.
Inessential but fun case of an elected official saying very much the wrong thing.
Not Covid
Reminder, purely about actual cars:
Remember that if you own an Oculus, and your Facebook account gets suspended because of reasons (such as saying facts that contradict local health authorities) you will lose all your games and save data permanently, no refunds, no fixes. Might want to consider a secondary Facebook account for this purpose, unless you’re using your Oculus to recover your Facebook account, which is also a thing.
In Scott’s recent post, he reckons with his struggles to not make mistakes despite the need to quickly produce a lot of content. I have this problem as well, and last week failed to check something I should have checked. My solution so far has essentially been to state my epistemic confidence in my statements, and to carefully put conditionals on statements that I haven’t verified. So last week I wrote “I am not aware of any X” and it turns out there are a bunch of common Xs and I really should have known that already and also should have checked even though I didn’t know, but I did know I hadn’t checked so I wrote I wasn’t aware. I ended up editing the paragraph (on pregnancy) a few times. There wasn’t anything false when I wrote it but once it was pointed out it obviously needed to be fixed quickly. This occasionally happens, also there are occasional typos, broken links and other stupid mistakes, and occasionally one of the sources turns out to be fake, as was the case with a British account a while back.